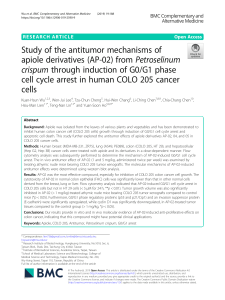
TUGAS MATA KULIAH ILMU BEDAH KHUSUS VETERINER “TEKNIK OPERASI COLOTOMY DAN COLECTOMY” OLEH : Putu Angga Prasetyawan 1609511052 Putu Ayu Dina 1609511054 Aurellia Dewi Rosalina Adeliriani 1609511055 Putu Jodi Wiraguna Tangkas 1609511057 LABORATORIUM BEDAH VETERINER FAKULTAS KEDOKTERAN HEWAN UNIVERSITAS UDAYANA 2019 KATA PENGANTAR Puji syukur kami panjatkan kehadirat Tuhan Yang Maha Esa atas segala limpahan rahmat dan hidayah-Nya sehingga Paper “Teknik Operasi Colotomy dan Colectomy” ini dapat diselesaikan tepat waktu. Makalah ini dibuat dalam rangka menyelesaikan tugas yang akan dijadikan landasan dalam penilaian softskill pada proses pembelajaran Mata Kuliah Ilmu Bedah Khusus Veteriner Fakultas Kedokteran Hewan Universitas Udayana. Ucapan terima kasih dan penghargaan yang setinggi-tingginya kami sampaikan kepada dosen pengajar yang telah memberikan banyak bimbingan dan arahan kepada kami dalam penyusunan makalah ini. Tidak lupa penulis juga mengucapkan terima kasih kepada semua pihak yang telah membantu dan memberikan dukungan pada kami. Kami menyadari bahwa tulisan ini masih banyak kekurangan baik dari segi materi, ilustrasi, contoh, maupun sistematika penulisan. Oleh karena itu, saran dan kritik dari para pembaca yang bersifat membangun sangat kami harapkan. Besar harapan kami karya tulis ini dapat bermanfaat baik bagi pembaca pada umumnya terutama bagi dunia kedokteran hewan di Indonesia. Denpasar, 27 Oktober 2019 Penulis i DAFTAR ISI KATA PENGANTAR ........................................................................................ i DAFTAR ISI ...................................................................................................... ii BAB I PENDAHULUAN 1.1 Latar Belakang ......................................................................................... 1 1.2 Rumusan Masalah……............................................................................. 2 1.3 Tujuan Penulisan ...................................................................................... 2 1.4 Manfaat Penulisan…………………………………………………......... 2 BAB II PREOPERASI DAN ANASTESI 2.1 Pre Oprasi.................................................................................................. 3 2.2 Premedikasi dan Anastesi ......................................................................... 4 BAB III PROSEDUR OPERASI 3.1 Prosedur Operasi Colotomy……………………………………………... 5 3.2 Teknik Operasi Colectomy……………………………………………… 7 BAB IV HASIL DAN PASCA OPERASI 4.1 Perawatan Pasca Operasi Colotomy dan Colectomy…………………………….... 9 BAB V PENUTUP 5.1 SIMPULAN ............................................................................................. 10 5.2 SARAN .................................................................................................... 10 DAFTAR PUSTAKA ......................................................................................... 11 ii DAFTAR GAMBAR Gambar 1. Proses pengeluaran colon dengan bantuan endoskopi…………. 5 Gambar 2. Megacolon pada anjing yang akan dilakukan colotomy……….. 6 Gambar 3. Proses pengeluaran isi colon…………………………………… 6 Gambar 4. Penguncian bagian batas atas dan bawah colon………………… 7 Gambar 5. Ligasi pembuluh darah sekitar colon…………………………… 8 Gambar 6. Proses pemotongan bagian colon yang diklemp Penutupan……….. 8 iii BAB I PENDAHULUAN 1.1 Latar Belakang Hewan kesayangan ataupun hewan ternak lainnya dapat mengalami gangguan pada saluran pencernaannya, terkhususnya colon. Gangguan yang dimaksud disini seperti bila terjadi sumbatan (obstruksi), dan perforasi pada colon sehingga menghambat proses keluarnya feses dari dalam usus besar. Selain itu dapat juga terjadi kasus dekompersi usus dan colon berukuran kecil. Kasus gangguan pada kolon dapat ditangani dengan operasi bedah colotomy ataupun colectomy, tergantung dari permasalahan atau indikasi apa yang dialami pasien. Colotomy adalah tindakan bedah yang dilakukan untuk menginsisi bagian colon. Hal ini dilakukan untuk mengeluarkan benda asing, kotoran ataupun yang lainnya dari dalam colon yang menyebabkan obstruksi colon sehingga mengganggu sistem pencernaan ataupun menghambat proses keluarnya feses dari dalam usus besar. Sedangkan Colectomy adalah tindakan bedah yang dilakukan untuk memotong sebagian kolon (colecomy subtotal) atau seluruh bagian colon (colectomy total) tergantung dari besar-kecilnya kerusakan yang pada kolon tersebut. Colectomy subtotal adalah prosedur bedah yang diindikasikan untuk kasuskasus sembelit kronis non-responsif terhadap intervensi medis. Tujuan dari colectomy subtotal adalah untuk menghilangkan bagian colon yang mengalami kerusakan, sehingga menghasilkan feses yang lebih lembut, kotoran yang semisolid, yang kemudian dapat melewati pelvis yang mengalami penyempitan. Setelah colectomy subtotal atau total, kompensasi vili akan meningkat, begitu pula dengan ketinggian dan density enterocyte juga meningkat, feses biasanya menjadi lebih lembut pada 3 bulan pertama setelah operasi. Namun secara klinis, fungsi usus masih berada dalam keadaan normal. 1 1.2 Rumusan Masalah 1. Apa definisi dari episiotomi dan episiostomi? 2. Bagaimana prosedur pre-operasi episiotomi dan episiostomi? 3. Bagaimana prosedur operasi episiotomi dan episiostomi? 4. Bagaimana penanganan pascaoperasi episiotomi dan episiostomi? 1.3 Tujuan Penulisan Tujuan dari dibuatnya paper ini yaitu agar mahasiswa dapat mengerti dan memahami : 1. Definisi dari episiotomi dan episiostomi. 2. Prosedur pre-operasi episiotomi dan episiostomi. 3. Prosedur operasi episiotomi dan episiostomi. 4. Penanganan pascaoperasi episiotomi dan episiostomi. 1.4 Manfaat Penulisan Manfaat dari dibuatnya paper ini untuk mengetahui dan bisa mengaplikasikan episiotomi dan episiostomi. Memahami perbedaan mendasar anatar episiotomi dan episiostomi. 2 BAB II PRE OPRASI DAN ANASTESI 2.1 Pre Operasi Persiapan sebelum operasi dimulai dengan mempersiapkan operator, alat dan bahan operasi, pasien serta ruangan operasi. Alat dan bahan yang digunakan meliputi alat dan bahan yang merupakan kebutuhan umum pada operasi seperti scalpel, gunting, jarum, spuit, iodine, obat-obatan premedikasi dan anastesi, dan semua alat penunjang pada meja operasi. Operator disiapkan secara mental dan psikologis untuk melakukan operasi. Pasien atau hewan disiapkan dengan cara disterilkan bagian yang akan dilakukan operasi dengan mencukur bulu. Peneguhan diagnosa agar memastika tataletak maupun posisi benda asing dapat menggunkana USG maupun foto Rontgen. Usia, jenis, jenis kelamin, tanda-tanda klinis (misalnya, kesan umum, peredaran darah dan parameter pernapasan, tanda-tanda perut, tenesmus dan konstipasi), durasi tanda-tanda klinis, data laboratorium (hematologis dan penilaian biokimiawi), perioperative acara dan klinikopatologis Temuan dicatat. Tindak lanjut jangka panjang didasarkan (1) pada review dari catatan klinis dan (2) di telepon wawancara dengan pemilik. (Nameth, 2008). Pada pre operasi untuk memperbaiki keseimbangan elektrolit dan energy, pasien perlu dirawang denga diberikan larutan-larutan seperti Laktat Ringer (500 ml), 5% Larutan glukosa (500 ml), dan larutan Aminosteril (30ml) (Abedi, 2012). Selain itu, 2—3 sebelum operasi berlangsung, sehari sekali hewan diberikan antibiotic dan vitamin untuk menunjang operasi tersebut. Dapat diberikan Penisilin 800.000 UI secara IV dan vitamin B-com 3-5 ml secara IV. Menurut penelitian (Nameth, 2008) pasien dapat diberikan treatmen antibiotic secara parenteral dengan 10 mg / kg amoksisilin / asam klavulanat, ditambah 30 mg/kg enrofloxacin. 3 2.2 Premedikasi dan Anastesi Anastesi yang digunakan adalah anastesi umum. Sebelumnya hewan diberikan juga premedikasi. Pemberian anastesi dan premedikasi dapat beragam dari campuran beberapa obat-obatan anastesi. Premedikasi yang diberikan dapat berupa atropine (0.02-0.04 mg/kg) ataupun kombinasi atropine dan acepromazine (0.1-0.2 mg/kg) yang diberikan secara subkutan. Dapat juga diberikan berupa 0.01 mg/kg IV acepromazine dan 0.05 mg/kg IV fentanyl. Anastesi yang diberikan dapat berupa Ketamine HCl (4-6 mg/kg IM), atau bisa juga dengan 4 mg/kg Propofol. Untuk menjaga kesetabilan anastesi dan sebagai kontrol dapat diberikan kombinasi oxygen dan isofluren ataupun hanya isofluren tunggal (Nameth, 2008). Semua dosis diatas merupakan dosis yang diberikan untuk anjing. 4 BAB III PROSEDUR OPERASI 3.1 Prosedur Operasi Colotomy Penentuan lokasi pembedahan dapat ditentukan menggunakan alat bantu yaitu alat endoskopi , yang dimana alat endoskop ini memiliki kamera dan juga senter untuk melihat keadaan organ di dalam tubuh. Alat endoskopi pada operasi Colotomy ini digunakan untuk eksplorasi cavum abdomen untuk menemukan colon Gambar 1. Proses pengeluaran colon dengan bantuan endoskopi Sumber: Bustamante-Lopez et al., 2016 Jika posisi colon menggunakan endoskopi , lakukanlah penandaan pada kulit yang sudah ditentukan dapat dilakukan incisi pada bagian ventral abdomen sesuai dengan lokasi yang tepat / yang di tandai. Jika abdomen sudah terbuka, bagian colon dapat diangkat ke permukaan untuk mempermudah proses pengeluaran. 5 Gambar 2. Megacolon pada anjing yang akan dilakukan colotomy. Sumber: Abedi et al., 2012 Berikan stay suture pada bagian yang akan dibedah sebagai patokan atau penanda agar tidak berpindah. Lakukan incisi perlahan, lalu arahkan luka incisi pada wadah tampung guna menampung seluruh isi colon, aplikasikan dengan bersih guna mencegah adanya beberapa partikel yang masuk kedalam cavum abdomen. Gambar 3. Proses pengeluaran isi colon. Sumber: Abedi et al., 2012 Tutup bekas incisi dengan benang absorable secara simple continuous pada mukosa dan dilanjutkan dengan lambert suture pada sisi bagian luar. Reposisi colon dan tutup kembali abdomen dari peritoneum, subcutan sampai kutan. Penutupan sayatan dilakukan dengan jahitan yang absorbable simple 6 continous, diikuti oleh jahitan jenis cushing interrupted pada baris kedua. Kemudian colon dijahit dengan 4 jahitan mattress horizontal ke otot kiri psoas mayor dan minor di dekat aauda kaudal dan kaudal vena cava. Rongga perut ditutup dengan teknik standar simple interrupted menggunakan benang non absorbable (Abedi et al., 2012). 3.2 Teknik Operasi Colectomy Pembedahan colectomy juga dapat dilakukan dengan bantuan alat endoskopi seperti pada colotomy. Eksplorasi cavum abdomen dan identifikasi colon. Langkah pertama yang dilakukan membuat incisi pada bagian ventral abdomen yang tepat sesuai dengan bantuan alat endoskopi. Colon yang sudah teridentifikasi dapat diangkat keluar permukaan tubuh. Kunci bagian batas atas colon (ilio colon junction) dan bagian bawah colon (colo rectal junction) dengan menggunakan forcep klemp dengan jarak beberapa segmen. Gambar 4. Penguncian bagian batas atas dan bawah colon Ligasi semua pembuluh darah sekitar colon dan semua vena mesenterika yang berada pada colon. Jika ligasi sudah dilakukan, pemotongan bagian colon dapat dilakukan. Gunting bagian colon yang akan diangkat dari mesenterium. 7 Gambar 5. Ligasi pembuluh darah sekitar colon Gunting bagian colon yang telah diklemp mengunakan mentzbaum dan temukan kedua bagian. Sambungkan rektum-illium dengan jahitan simple interrupted. Untuk bagian rektum yang lebih diberi jahitan lambert. Gambar 6. Proses pemotongan bagian colon yang diklemp Penutupan Abdomen pada colectomy dilakukan sama seperti pada colotomy. Reposisi colon yang sudah dibedah dan tutup kembali abdomen dari peritoneum, subkutan sampai kutan. Penutupan sayatan dilakukan dengan jahitan yang absorbable simple continous, diikuti oleh jahitan jenis cushing interrupted pada baris kedua. Kemudian usus besar dijahit dengan 4 jahitan mattress horizontal ke otot kiri psoas mayor dan minor di dekat aauda kaudal dan kaudal vena cava. Rongga perut ditutup dengan teknik standar simple interrupted menggunakan benang non absorbable (Abedi et al., 2012). 8 BAB IV HASIL DAN PASCA OPERASI 4.1 Perawatan Pasca Operasi Colotomy dan Colectomy Paca operasi Hewan dimonitor perkembangannya tiap 3 jam. Daerah incisi dibersihkan dan diolesi dengan iodium tincture 3%. ke dalam daerah bekas operasi disemprotkan penisilin oil, kemudian hewan diberi penisilin G dengan dosis 4000 – 10.000 IU/kgBB dan vitamin B-complex secara IM disertai pemberian antiinflamasi nonsteroid. Antibiotik spectrum luas diberikan sampai 48 jam pasca operasi. Penutupan dengan perban juga dilakukan pada bekas insisi di abdomen. Hewan juga diberi cairan infus secara IV sebanyak 40-60ml/kgBB dan buprenorfin (Buprecare; Animalcare) selama 24 jam setelah operasi dengan metronidazole (Metronidazole; Marco Pharma) dan amoksisilin / klavulanat (Augmentin; GlaxoSmithKline Inggris) dilanjutkan selama 5 hari. (Darren C. 2012.) Pemberian minum air hangat dilakukan beberapa jam setelah operasi dan harus diulang tiap setengah jam (maintenance: 20L/450 kg BB/hari). Jangan diberi makan hingga 12-24 jam pasca operasi, Pakan dalam jumlah sedikit dapat diberikan sesegera mungkin jika hewan sudah mau makan dengan sendirinya dengan diberi suplemen lemak untuk meningkatkan kalori. Setelah 30 hari, hewan sedikit demi sedikit diberikan exercise. 9 BAB V PENUTUP 5.1. Kesimpulan Colotomy adalah pembedahan untuk membuka usu besar yaitu pada bagian colon , dimana bertujuan untuk mengeluarkan benda asing atau tumor atau hal hal yang abnormal / tidak seharusnya pada colon. Colectomy merupakan pengangkatan sebagian organ colon yang mengalami kerusakan atau abnormalitas pada organnya sehingga harus di potong / di angkat. 5.2. Saran Penulis berharap mahasiswa mampu memahami dan mengerti dan bisa membedakan apa yang dimaksud dengan colotomy dan colectomy dan juga mengetahui teknik operasi colotomy dan colectomy. 10 DAFTAR PUSTAKA Abedi, Gholamreza., Asghari, A., Alizadeh, Rahim., Shayan, Navid. 2012. Colon Surgical Stabilization on Psoases Muscles for Treatment of Megacolon in Dog. Department of Surgery, Faculty of Veterinary Medicine, Science and Research Branch, Islamic Azad University, Tehran, Iran . Barnes, Darren C. 2012. Subtotal colectomy by rectal pull-through for treatment of idiopathic megacolon in 2 cats : case report. Can Veterinary J. United Kingdom. Bustamante-Lopez, L. A., Sulbaran, M., Nahas, S. C., de Moura, E. G. H., Nahas, C. S., Marques, C. F., Sakai, C., Ceconello, I., Sakai, P. 2016. Endoscopic colostomy with percutaneous colopexy: an animal feasibility study. Department of Gastroenterology. Surgical Division. University of São Paulo Medical School. São Paulo, Brazil. Nemeth T., Solymosi And N., Balka G. 2008. Long-term results of subtotal colectomy for acquired hypertrophic megacolon in eight dogs. Journal of Small Animal Practice (2008). 49, 618–624 11 LAMPIRAN JOURNAL 12 Global Veterinaria 9 (2): 232-236, 2012 ISSN 1992-6197 © IDOSI Publications, 2012 DOI: 10.5829/idosi.gv.2012.9.2.6541 Colon Surgical Stabilization on Psoases Muscles for Treatment of Megacolon in Dog 1 Gholamreza Abedi, 1Ahmad Asghari, 1Rahim Alizadeh and 2Navid Shayan Department of Surgery, Faculty of Veterinary Medicine, Science and Research Branch, Islamic Azad University, Tehran, Iran 2 Graduated from the Faculty of Veterinary Medicine, Garmsar Branch, Islamic Azad University, Garmsar, Iran 1 Abstract: Megacolon refers to an abnormal dilatation of the colon. Although it seems to be more common in cats, megacolon may also occur in dogs. This study included fourteen large-breed dogs affected with megacolon, aged 6 - 11 years. Colotomy and colopexy were performed in all dogs. The results of this study showed that symptoms do not improve in five dogs and so they were needed to subtotal colectomy surgery. Also, due to late referral and old age two other dogs were died. Seven dogs were successfuly recovered with colopexy. The aim of colopexy in this study is to create a direct way for the transit of stool in the colon and also removal the angle between the damaged and healthy colon which is created at the pelvic cavity inlet. Furthermore, the contractions of vascular (caudal aorta and caudal vena cava) and muscles area stimulate colon movements. Key words: Megacolon Psoases Muscles Dog INTRODUCTION On the other hand, hypertrophic megacolon refers to the functional disorder that develops as a result of chronic obstructive lesions (stenosis of the pelvic canal, tumor, foreign body, etc.) [4]. The therapy for megacolon depends on several factors including the severity of constipation and fecal impaction and the underlying cause. The initial treatment is aimed to establish and/or maintains a fluid and electrolyte balance, as well as to eliminate the possible causes of constipation. In addition, medical therapy with stool softeners is the first-line treatment for this condition. In this respect, animals should be appropriately hydrated and then an enema should be performed. Thereafter, medical management with laxatives should be initiated. Intestinal transit and other motility disorders in both dogs and cats [5, 6]. When medical therapy is no longer effective, surgery is recommended. Although surgery is usually referred to as a subtotal colectomy, in some cases colonotomy with fecal mass removal may also be considered as the treatment of choice [7]. Postoperatively, parenteral antibiotic and vitamin therapy should be continued. Prognosis depends on early recognition and management of megacolon [8]. This study is an evaluation of colopexy in treatment of megacolon to prevent removal of the colon The large intestine is responsible for absorption of water and salt and the storage of feces. The large intestine is relatively short in dogs and cats, approximately 10 - 20% of the length of the small intestine, reflecting the fact that the large intestine plays a less significant role in nutrient digestion [1]. Megacolon is a condition that is uncommonly described in dogs. It refers to an abnormal dilatation of the colon that may be acute, chronic or toxic. Chronic megacolon can be classified as congenital (also known as Hirschsprung's disease in humans) or acquired and may be either primary or secondary. The cause of primary megacolon is unknown, so it is also termed idiopathic. The pathogenesis of idiopathic megacolon is still a subject of controversy, although it has been historically attributed to a primary neurogenic or degenerative neuromuscular disorder [2]. Secondary megacolon can occur as the result of intestinal wall lesions or various conditions that prevent defecation for a prolonged period of time [3]. Two pathological mechanisms are implicated in megacolon development: dilatation and hypertrophy. Dilated megacolon represents the end-stage of colonic dysfunction in idiopathic cases. Corresponding Author: Ahmad Asghari, Faculty of Veterinary Medicine, Department of Surgery, Science and Research Branch, Islamic Azad University, Tehran, Iran. Mob: +98-9144147924. 232 Global Veterinaria, 9 (2): 232-236, 2012 Fig1: Psoas major & minor muscle and the recurrence of megacolon, because one of the reasons of subtotal colectomy is the prevention of megacolon recurrence. Instead of removing the colon in colopexy, first colotomy is conducted and then the colon is fixed in the lumbar muscle (Psoas major & minor) (Figure 1), because the accumulation of feces in the distended colon and increase of the volume and weight of the feces, the colon is oriented toward the bottom of the abdominal cavity and an angle near 90 degrees is created between the affected and normal colon in the pelvic cavity inlet that prevents the movement of feces into the rectum. If the angle can be omitted by fixing colon in lumbar, it is possible to prevent from recurring megacolon due to the created direct path. Fig 2: Radiographic image of dilated colon MATERIALS AND METHODS This study included 14 large-breed dogs affected with megacolon, aged 6-11 years. After recording the profile of all dogs and the diagnosis of megacolon using the clinical examination and abdominal radiographic findings, colotomy and colopexy was performed in all dogs. Abdominal radiography of all examined dogs before surgery showed colonic distension with stool retention. Dilated colon was evident on all radiographic images (Figure 2). In most cases, enlarged colon extended from the epigastric region to the pelvic canal. Fig. 3: Gross appearance of megacolon before and after colotomy Preoperative Care: Immediately after the diagnosis was established, over a period of 2 - 3 days, all dogs were subjected to an initial treatment for restoration of their general health condition and for surgical procedure preparation. In order to correct electrolyte and energy imbalance, the animals were treated with infusions of Ringer's lactate solution (500 milliliter), 5% glucose solution (500 ml) and aminosteril solution (30 ml). In addition, once a day for three days, all animals were treated with preoperative antibiotics and vitamin therapy (penicillin G, 800,000 International unit Intra Venous; vitamin B-complex, 3-5 ml Intra Muscular). Before surgery, the animals were premedicated with atropine sulphate (subcutaneous) and acepromazine (IV) and then anesthetized with ketamine hydrochloride (IM) and maintained with isoflurane inhalation. Surgical method; all animals underwent a median laparatomy. After pulling out the colon, extra-abdominal incision was created in the anti-mesenteric border of colon and followed by manual extraction of the intestinal contents (Figure 3). Closure of the incision was accomplished by a continuous absorbable, synthetic, braided suture (polyglactin 910 3-0), followed by a second row interrupted cushing type suture. Then the colon was sutured by 4 horizontal mattress sutures to the left psoas 233 Global Veterinaria, 9 (2): 232-236, 2012 major & minor muscles near the caudal aorta and caudal vena cava. After lavage the abdominal cavity, the abdomen was closed with standard technique. Postoperative Care: All dogs during the postoperative period (8 days after surgery), antibiotics, electrolyte solutions and vitamin therapy (penicillin G, Ringer's lactate and vitamin B-complex) were continued and dogs were closely monitored for infection. The animals were deprived of water for two days after surgery. On the third postoperative day, all animals were given water only (3 x 150 mL). In addition to water, for the next four days (4th - 8th postoperative day), animals were fed with chicken soup (2 x 200 mL, concentrate). Thus, the daily amount of fluid, given per os, was 1 liter. During this period, the animals were deprived of solid food. Eight days after surgery, both medicament and vitamin therapy were interrupted. Starting from the 9th postoperative day, solid food (raw minced beef 2 x 150 g and corn bran 2 x 50 g, per day) was introduced to the diet and dogs were allowed access to water. During the third postoperative week, in addition to raw beef, fresh bread (2 x 50 g, per day) was introduced to the diet. In all animals were given an increased amount of food (meat 2 x 200 g, bread 2 x 50 g, corn bran 50 g and soup concentrate 2 x 200 mL). Animals were fed twice a day, during the period of 30 days after surgery. The Elizabethan collar was placed around the animal's neck to prevent them from licking or biting wounds. Skin sutures were removed on the 12th postoperative day, while the protective collar was removed three days later. Fig. 4: Radiographic image after colopexy of colon DISCUSION Patients with intractable constipation can be divided into those with normal gut diameter and those with a dilated gut. The former includes slow-transit constipation, pelvic outlet obstruction and the latter includes congenital megacolon (Hirschsprung disease), colonic pseudo-obstruction and acquired megacolon. The pathophysiology of constipation in these entities is poorly understood, although there have been several investigations on this matter [3, 9- 13]. It was previously thought that megacolon commonly affects older cats. However, recent studies show that both feline and canine megacolon may be seen at any age [14]. According to a review of 120 cases published in English veterinary literature, most cases of megacolon are observed in middle-aged, male cats (70%). These data also suggest that megacolon commonly affects domestic shorthair (46%), domestic longhair (14%) and Siamese breeding [4]. An extensive list of differential diagnosis for the obstipated cat includes numerous factors associated with a prolonged constipation, such as: neuromuscular, Evaluation Methods: Appetite and feces of all dogs were evaluated for 30 days. 30 days after surgery, all dogs were submitted to radiographic evaluation. RESULTS The results of this study showed that symptoms do not improve in five dogs and so they were needed to subtotal colectomy surgery. Also, due to late referral and old age two other dogs died. At all seven dogs recovered due to doing colopexy and 20 days after surgery had a good appetite. Comparison of fecal in all dogs showed 7 dogs had normal fecal 10 days after surgery. Radiographic evaluation results showed that the descending colon lumen diameter decreased in all dogs with colopexy surgery (Figure 4). 234 Global Veterinaria, 9 (2): 232-236, 2012 mechanical, metabolic, endocrine, inflammatory and environmental factors. Although in some cases differential diagnosis may be of critical importance the majority of cases of obstipation are accounted for idiopathic megacolon (62%), pelvic canal stenosis (23%), nerve injury (6%) or Manx sacral spinal cord deformity (5%). In addition, in a small number of cases, obstipation was a result of complications of colopexy (1%) or colonic neoplasia (1%), while hypoganglionosis/ aganglionosis was suspected in 2% of cases, but not proven [4, 14]. However, the importance of differential diagnoses for the obstipated dog is not well documented. The goal of treatment is to maintain a soft stool and to improve colonic motility. Recent studies confirmed that feline megacolon is characterized by a generalized dysfunction of colonic smooth muscle and that treatments aimed at stimulating colonic smooth muscle contraction might improve colonic motility [15]. In cats the disease is characterised by repeated episodes of constipation or prolonged obstipation that may result in complete absence of defecation. Affected cats are presented with anorexia, dehydration, weight loss, vomiting and lethargy. Occasionally, chronically constipated cats have intermittent episodes of diarrhea. Cats affected with idiopathic dilated megacolon usually have a history of recurrent constipation culminating in obpstipation. On the contrary, animals affected with hypertrophic megacolon usually have a history of automobile or other trauma [16, 17]. Several surgical techniques for the management of feline megacolon have been described, including coloplasty and partial or subtotal colectomy [18]. The aim of colopexy in this study is to create a direct way for the transit of stool in the colon and also removal the angle between the damaged and healthy colon which is created at the pelvic cavity inlet. Furthermore, the contractions of vascular (caudal aorta and caudal vena cava) and muscles area stimulate colon movements. Diet was also an important part of postoperative treatment. Constipated patients are usually fed a standard diet high in fiber to help attract water to the stool, improving its consistency. Consumption of high-fiber foods contributes to optimal surgery outcome and helps to prevent postoperative constipation. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. REFRENCES 1. 13. Guilford, G.W., 1996. Nutritional management of gastrointestinal disease. In: Strombeck’s Small Animal Gastroenterology, Eds. Guilford, G.W.S.A. Center, D.R. Strombeck, D.A. Williams and D.J. Meyer, W.B. Saunders, 3rd ed, pp: 889-910. 235 Meier-Ruge W.A., H. Müller-Lobeck, F. Stoss and E. Bruder, 2006. The pathogenesis of idiopathic megacolon. Eur. J. Gastroenterol Hepatol, 18: 1209-1215. Bharucha, A.E. and S.F. Philips, 1999. Megacolon: acute, toxic and chronic. Curr Treat Options Gastroenterol, 2: 517-523. Washabau, R.J. and A.H. Hasler, 1996. Constipation, obstipation and megacolon. In: Consultations in Feline Internal Medicine, Ed. August, J.R. W.B. Saunders, 3rd ed, pp: 104-113. Wiselman, L.R. and D. Faulds, 1994. Cisapride. An updated review of its pharmacology and therapeutic efficacy as a prokinetic agent in gastrointestinal motility disorders. Drugs, 47: 116-152. Washabau, R.J., 2003. Gastrointestinal motility disorders and gastrointestinal prokinetic therapy. Vet Clin. North. Am. Small. Anim. Pract, 33: 1007-1028. Webb, S.M., 1985. Surgical management of acquired megacolon in cat. J Small Anim Pract, 26: 399-405. Nemeth, T., N. Solymosi and G. Balka, 2008. Long-term results of subtotal colectomy for acquired hypertrophic megacolon in eight dogs. J. Small Anim Pract, 12: 618-624. Galvez, Y., R. Kaba, R. Vajtrova, A. Frantlova and J. Herget, 2004. Evidence of secondary neuronal intestinal dysplasia in rat model of chronic interstinal obstruction. J. Investig Surg, 17: 31-39. Lee, J.I., H. Park, M.A. Kamm and I.C. Talbot, 2005. Decreased density of interstitial cells of Cajal and neuronal cells in patients with slow-transit constipation and aquired megacolon. J. Gastroenterol. Hepatol, 20: 1292-1298. Matsuda, H., J. Hirato and M. Kuroiwa 2006. Nakayato, H i st o p at h o l o g i c al an d immunohistochemical study of the enteric innervations among arious types of aganglionoses including isolated and syndromic Hirschsprung disease. Neuropathology, 26: 8-23. Da Silveira, A.B.M. D. D’Avila Reis, E.C. Oliveira, S.G. Neto, A.O. Luquetti and D. Poole, 2007a. Neurochemical coding of the enteric nervous system in chagasic patients with megacolon. Dig. Dis. Sci., 52: 2877-2883. Da Silveira, A.B., E.M. Lemos, S.J. Adad, R. Correa-Oliveira, J.B. Furness and D. D’Avila Reis, 2007b. Megacolon in Chagas disease: a study of inflammatory cells, enteric nerves and glial cells. Hum Pathol, 38: 1256-1264. Global Veterinaria, 9 (2): 232-236, 2012 14. Washabau, R.J. and J.A. Hall, 1997. Diagnosis and management of gastrointestinal motility disorders in dogs and cats. Compend Contin Educ. Pract. Vet., 19: 721-737. 15. Washabau, R.J. and I.H. Stalis, 1996. Alterations in colonic smooth muscle function in cats with idiopathic megacolon. Am. J. Vet. Res., 57: 580-587. 16. Burrows, C.F., 1996. Constipation, obstipation and megacolon in the cat. Waltham Internat Foc., 6: 9- 14. 17. Washabau, R.J. and D. Holt, 1999. Pathogenesis, diagnosis and therapy of feline idiopathic megacolon. Vet Clin North Am Small Anim Pract, 29: 589-603. 18. White, R.N., 2002. Surgical menagment of constipation. J. Fel. Med. Sur., 4: 129-138. 236 1130-0108/2017/109/4/273-278 Revista Española de Enfermedades Digestivas © Copyright 2017. SEPD y © ARÁN EDICIONES, S.L. Rev Esp Enferm Dig 2017, Vol. 109, N.º 4, pp. 273-278 ORIGINAL PAPERS Endoscopic colostomy with percutaneous colopexy: an animal feasibility study Leonardo Alfonso Bustamante-Lopez, Marianny Sulbaran, Sergio Carlos Nahas, Eduardo Guimaraes Horneaux de Moura, Caio Sergio Nahas, Carlos Federico Marques, Christiano Sakai, Ivan Ceconello and Paulo Sakai Department of Gastroenterology. Surgical Division. University of São Paulo Medical School. São Paulo, Brazil ABSTRACT Background: Indications for colostomy in colorectal diseases are obstruction of the large bowel, such as in cancer, diverticular disease in the acute phase, post-radiotherapy enteritis, complex perirectal fistulas, anorectal trauma and severe anal incontinence. Some critically ill patients cannot tolerate an exploratory laparotomy, and laparoscopic assisted colostomy also requires general anesthesia. Objective: To evaluate the feasibility, safety and efficacy of performing colostomy assisted by colonoscopy and percutaneous colopexy. Materials and methods: Five pigs underwent endoscopic assisted colostomy with percutaneous colopexy. Animals were evaluated in post-operative days 1, 2, 5 and 7 for feeding acceptance and colostomy characteristics. On day 7 full colonoscopy was performed on animals followed by exploratory laparotomy. Results: Average procedure time was 27 minutes (2154 min). Postoperative mobility and feeding of animals were immediate after anesthesia recovery. Position of the colostomy, edges color, appearance of periostomal area, as well as its function was satisfactory in four animals. Retraction of colostomy was present in one pig. The colonoscopy and laparotomy control on the seventh day were considered as normal. A bladder perforation that was successfully repaired through the colostomy incision occurred in one pig. The main limitation of this study is its experimental nature. Conclusion: Endoscopic assisted colostomy with percutaneous colopexy proves to be a safe and effective method with low morbidity for performing colostomy in experimental animals, with possible clinical application in humans. Key words: Colostomy. Endoscopy. Colopexy. INTRODUCTION A colostomy is a surgical procedure that aims to divert the fecal stream to the outside through an orifice made in the abdominal wall, which may be temporary or permanent (1). Colorectal surgical procedures have been performed via minimally invasive techniques with increasing frequency (2). Although colostomy has traditionally required forReceived: 05-03-2016 Accepted: 22-12-2016 Correspondence: Leonardo Alfonso Bustamante-Lopez. Department of Gastroenterology. Surgical Division. University of São Paulo Medical School. São Paulo, Brazil e-mail: [email protected] mal laparotomy, this procedure could be performed via an trephine, endoscopic or laparoscopic approach (3-8). Endoscopic-assisted colostomy without general anesthesia and laparotomy was first reported by Mattingly and Mukerjee (3). However, percutaneous colopexy facilitates fixation of the colon to the abdominal wall on its anti-mesenteric side, adding important benefits. The indications for the use of colostomy in colorectal diseases are colon, rectum or anus obstruction, diverticular disease in the acute phase, post-radiation enteritis, complex perirectal fistula, anorectal trauma, severe anal incontinence, non-healing sacral decubitus ulcers in patients with spinal cord injury, complicated anal Crohn’s disease, recurrent rectovaginal fistula, pelvic floor dysfunction, and a dehisced coloanal anastomosis (2). This procedure is often necessary in critically ill patients who may not be able to tolerate a laparotomy or general anesthesia. The aim of this study is to evaluate the feasibility, safety and efficacy of performing colostomy under colonoscopic visualization and the use of colopexy without additional morbidity of abdominal exploration and general anesthesia in laboratory animals. METHODS This was a prospective, experimental, phase-I, survival animal study. The study was conducted between May and July 2014 at the Experimental Surgery Unit, University of São Paulo Medical School, Brazil. The study was approved by the Institutional Animal Care and Use Committee of the University of São Paulo Medical School, and conducted in accordance with current legislation with regard to the care and use of laboratory animals. Animal preparation Five healthy domestic female Yorkshire race pigs were used. Animals had an average pre-procedure weight of 35 kg (range 31.4 to Bustamante-Lopez LA, Sulbaran M, Nahas SC, Guimaraes Horneaux de Moura E, Nahas CS, Marques CF, Sakai C, Ceconello I, Sakai P. Endoscopic colostomy with percutaneous colopexy: an animal feasibility study. Rev Esp Enferm Dig 2017;109(4):273-278. DOI: 10.17235/reed.2017.4201/2016 274 L. A. BUSTAMANTE-LOPEZ ET AL. 40.8 kg), and no previous surgery. Pigs were prepared at the experimental laboratory of the Clinics Hospital Complex, University of São Paulo Medical School. Animals were kept fasting 24 hours before the intervention, and received an enema one hour before the procedure to clean the rectum and distal colon. In the lithotomy position with opened legs, all animals were submitted to tracheal intubation and mechanical ventilation, and maintained under general anesthesia with Ketamine Base® (intravenous 5 mg/kg) and Thiopental® (intravenous 10-30 mg/kg), followed by inhalation of Isoflurane®. All animals were kept alive 7 days after intervention for follow up. Colostomy technique Standardization of the technique was achieved by procedures performed in a pilot protocol prior to initiating the study. Rev Esp Enferm Dig Colonoscopic examinations were performed by a single endoscopist with advanced skills. Colostomies were done by an experienced colorectal surgeon. The following steps were followed: 1. Transanal introduction to the descending colon with a gastroscope (Pentax EG - 290) (Fig. 1). 2. Identification of the anterior colonic wall and the best site for trans-illumination on the abdominal wall, suitable for colopexy (Fig. 1). 3. Cleansing and anti-sepsis of the abdominal wall with povidone-iodine and saline. 4. Puncture of the abdominal wall at the previously identified best place for trans-illumination with the Loop Fixture II Gastropexy Kit® (Fig. 2). In brief, this device has two needles, one which has a suture inserted immediately before the tip of the needle, and the other which has a suture-holding loop placed on it (Fig. 2). Fig. 1. Fig. 2. Rev Esp Enferm Dig 2017;109(4):273-278 2017, Vol. 109, N.º 4 ENDOSCOPIC COLOSTOMY WITH PERCUTANEOUS COLOPEXY: AN ANIMAL FEASIBILITY STUDY 5. Under endoscopic visualization, the suture-holding needle was pushed down to form a loop for holding the suture (Fig. 3). 6. The suture was advanced down so that its distal end passed through the suture-holding loop. 7. After endoscopic visualization that the distal end of the suture had passed through the suture-holding loop, the loop was placed back in the puncture needle and pushed down to form a loop to release the suture. The free suture was knotted against the abdominal wall to hold the colon to the parietal peritoneum. 9. The endoscope was further withdrawn and a small disc of skin was removed proximal to the colopexy. A loop colostomy was performed in the anti-mesenteric wall, and the proximal-to-distal orientation of the intestinal loop was clearly identified aided by the colonoscope (Fig. 4). 275 10. The colostomy was fixed by stitching the anterior colonic wall to the aponeurosis and subcuticular layer circumferentially with polyglactin 910 (vycril 2-0) (Fig. 5). Postoperative management Oral feeding and mobility were started when animals were completely awakened. All animals were carefully observed and examined during a seven-day follow-up period to evaluate any changes in general condition, behavior and eating habits. Animals received prophylactic antibiotic therapy and analgesia with dipirone 1 g intramuscular. During postoperative days 1, 2, 5 and 7, animal feeding and movements, presence of feces in the colostomy, color of the edges of the mucosa and sinking of the colostomy were evaluated. Fig. 3. Under endoscopic visualization, the suture-holding needle was pushed down to form a loop for holding the suture. Fig. 4. A loop colostomy was performed in the anti-mesenteric wall, and the proximal-to-distal orientation of the intestinal loop was clearly identified aided by the colonoscope. Rev Esp Enferm Dig 2017;109(4):273-278 Fig. 5. The colostomy was fixed by stitching the anterior colonic wall to the aponeurosis and subcuticular layer circumferentially with polyglactin 910 (vycril 2-0). 276 L. A. BUSTAMANTE-LOPEZ ET AL. On day 7 all animals were sedated to perform colonoscopy and an exploratory laparotomy. At colonoscopy, periostomal mucosa and colopexy were evaluated. Exploratory laparotomy confirmed the absence of peritonitis and peritoneal abscess, and allowed direct observation of intraperitoneal colostomy. Finally, animals were sacrificed. Rev Esp Enferm Dig tive colopexy in all animals. Exploratory laparotomies excluded the presence of a localized abscess or diffuse peritonitis (Fig. 5). Fixation of the colonic wall to the parietal peritoneum was excellent and colon integrity was confirmed. DISCUSSION Statistics Results were reported as descriptive statistics, with means and ranges for quantitative variables. RESULTS A pilot protocol was conducted to learn the steps of the technique, observing potential problems in order to improve the procedure efficacy. Five endoscopic colostomies were performed in five pigs. All procedures were completed as planned (Figs. 3 and 4). The average procedure time was 27 minutes (range 21-54 min). Diet tolerance and mobility of the animal began in the immediate postoperative period post anesthesia recovery and were satisfactory in all pigs. Color of the edges, appearance of periostomal skin and its function were satisfactory in all animals during the follow-up period as well. Mucocutaneous separation of the colostomy with preservation of the stoma function occurred in one animal, with no sinking or stenosis (Table I). Complications During the pilot protocol stage, ileal interposition with perforation occurred in one animal. It was successfully repaired by laparotomy conversion. The bladder was perforated in the third pig. This perforation was successfully closed through the same incision in which the colostomy was made afterwards. The procedure was simple and fixation of the colostomy to the aponeurosis fascia was performed, without difficulty and with minimal bleeding. Control colonoscopy on the seventh day confirmed the presence of normal mucosa around colostomy and effec- The jury is still out for establishing the most effective surgical strategy for patients with partial obstructive left colon cancer. Colostomy has been described as a first step of a two-stage surgery on these patients (1,9,10). Moreover, neoadjuvant chemotherapy for locally advanced rectal and anal cancer has expanded the indications of a minimally invasive approach for fecal diversion, as it may avoid an additional surgery and the need of general anesthesia, serving as a bridge to oncologic surgical resection (11). Self-expandable metallic stents (SEMS) have been introduced as part of the management of complete or partial obstructive colorectal cancer, in order to avoid a twostep emergent surgical procedure that includes a colostomy (12). A recent meta-analysis demonstrated that colorectal SEMS as a bridge to elective surgery compared to emergency surgery in left-sided colorectal cancer obstruction showed a better prognosis in terms of lower postoperative morbidity, higher primary anastomosis rate and lower stoma rate. Despite these favorable immediate postoperative outcomes, a similar overall postoperative mortality of SEMS insertion as a bridge to surgery compared to emergency surgery was shown (10.7% vs 12.4%) (13). Furthermore, the long-term oncological outcome, such as disease recurrence, was worse in the group with SEMS as a bridge to surgery than in the emergency surgery group. Based on these unfavorable long-term oncological outcomes, the recent SEMS guidelines by the European Society of Gastrointestinal Endoscopy (ESGE) do not recommend routine SEMS insertion as a bridge to surgery in potentially curable left-sided obstructive colorectal cancer (CRC) obstruction (14). Additionally, a higher risk of perforation in patients treated with SEMS that were receiving antiangiogenic agents such as bevacizumab has been reported (15). Therefore, endoscopic colostomy can emerge as a minimally invasive alternative that can serve as a bridge Table I. Post operative variables Pigs Feeding Presence of Feces Animal movements Colostomy mucosal color Complications Procedure weight (kg) Post procedure weight (kg) 1 Good Yes Yes Red No 37.3 37.1 2 Good Yes Yes Red No 31.4 31 3 Good Yes Yes Red Bladder perforation 40.8 40.3 4 Good Yes Yes Red No 32.4 32.5 5 Good Yes Yes Red Retraction 33.3 33.1 Rev Esp Enferm Dig 2017;109(4):273-278 2017, Vol. 109, N.º 4 ENDOSCOPIC COLOSTOMY WITH PERCUTANEOUS COLOPEXY: AN ANIMAL FEASIBILITY STUDY to oncologic treatment, potentially overcoming present limitations of SEMS without the additional morbidity of general anesthesia and surgery for fecal diversion. Technical advantages and limitations of different approaches to perform colostomy have been described. Laparotomy allows a thorough evaluation of the abdomen, but causes more pain, longer recovery time, and a larger scar. In addition, there is a higher chance of wound infection and incisional hernia (1,16). Minimally invasive techniques like laparoscopy, gasless or trephine technique avoid large abdominal incisions and therefore reduce postoperative pain, ileus, and wound complications (3-6). Other advantages may include shorter hospital stay, and earlier initiation of other treatment such as chemotherapy or radiation therapy in patients with locally advanced rectal or anal cancer. In the laparoscopic approach visualization is improved but costs are increased. Laparoscopy has been described as the best way to proceed for the formation of an intestinal stoma (17,18). In the gasless technique, there are no incisions other than the one that is done to create the stoma. Visualization is reasonable, recovery is faster, and pain is minimal. In addition, the procedure can be performed safely, with minimum morbidity. However, general anesthesia may be a drawback for critically ill patients (6,19). The trephine colostomy technique does not allow easy identification of the colon segment, and differentiation between the proximal and distal ends of the sigmoid loop can be technically difficult (7,20,21). Mattingly and Mukerjee first reported endoscopic-assisted colostomy without general anesthesia or laparotomy (3). Fifteen patients were involved in this study. Four cases were performed under local or regional anesthesia. Fecal stream was successfully diverted using this minimally invasive technique in all patients. No immediate perioperative complications related to this technique were described. However, a retrospective review of those patients reported retraction of the colostomy in 13% of cases (4). Although endoscopic-assisted colostomy is not a new technique (22,23), percutaneous colopexy adds important technical advantages: strong and permanent attachment of the colon to the abdominal wall facilitates safe colostomy performance. Besides that, a pexy stitch on the colonic mucosa serves as a reference to the point that must be overcome for the creation of a colostomy proximal to the pexy. This approach does not require the creation of a pneumoperitoneum and allows the creation of a colostomy under conscious sedation, with regional or local anesthesia. This probably could account for a lower risk of anesthesia complications, a shorter recovery time and, thus, lower costs of hospital care. In addition, procedural time is reduced. We reported an average procedure time of 25 minutes, compared to longer times reported with others techniques (6,17,22). Some of the patients who can benefit from this technique are those with important systemic comorbidities, Rev Esp Enferm Dig 2017;109(4):273-278 277 ASA III or IV, as it would prevent the use of general anesthesia. Moreover, neoadjuvant chemotherapy for locally advanced rectal and anal cancer has expanded the indications of a minimally invasive approach for fecal diversion, as it may avoid an additional surgery and the need of general anesthesia, serving as a bridge to treatment for oncologic resection (11,24). Bowel preparation was done with a rectal enema. That is because anterograde preparation is not feasible in most cases of partially obstructive tumors in humans. In some cases, the enema effect was not good enough and it was necessary to work with formed stool in the colon lumen. The endoscopist had no major problem to advance the scope over the feces. Considering that it is not a diagnostic procedure, we believe that working on a completely cleaned colon is not needed, favoring the use of the method in patients with partial colon or rectal obstruction. An important technical consideration regarding care for diminishing infectious risk is that the stoma is performed outside of the abdominal cavity, after having scope confirmation of the correct bowel segment to make the incision. Additionally, it is worth mentioning that a gastroscope was used instead of a colonoscope in order to reproduce the clinical scenario of having to overpass a stenosed rectal or colonic segment. Moreover the use of a slim gastroscope could be a reasonable option for this procedure in selected cases. Potential limitations of this technique are the small exposure of the incision with lack of intra-abdominal exploration and technical difficulty for aponeurosis fixation. The orientation of the endoscopist to reach the anterior abdominal wall is an obstacle that can be overcome by gentle palpation of the abdomen at the maximum trans-illumination point. This maneuver can be an obstacle in obese patients, but does not preclude the procedure. Besides, one of the major drawbacks of colostomy is shrinkage, and it is thought to be caused by mesenteric tension. Because of that we recommend that colostomy should be done between 20 and 30 cm from the anal verge, with the colonic wall directly against the abdominal wall and avoiding excess torque maneuvers of the scope. Of note, adequate patient selection should be considered, as multiple previous surgeries could preclude a successful mobilization and trans-illumination of the colon into the abdominal wall. With regard to possible causes for complications, important differences of pig anatomy compared to humans should be mentioned. The bladder can reach the umbilical scar in pigs. We think this anatomic variation could have influenced the bladder perforation on the third animal. On the other hand, the descending colon of the pig is found on the right side of the abdominal cavity, which could predispose the ileal interposition that we experienced during the pilot protocol stage. The different location of the descending colon also explains why colostomies in animals were performed on the right iliac fossa. 278 L. A. BUSTAMANTE-LOPEZ ET AL. Based on the need for alternatives to laparotomy and laparoscopy for the creation of ostomies, we made a technical breakthrough, and showed that endoscopic colostomy with percutaneous colopexy proves to be a simple, feasible and effective method with low morbidity for performing colostomy in experimental animals. Further studies will be needed to prove its successful clinical application in humans. 11. 12. 13. 14. REFERENCES 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. Fry RD, Mahmoud N, Maron DJ, et al. Colon and rectum. In: Townsend CM, Beauchamp RD, Evers BM, Mattox KL, eds. Sabiston Textbook of Surgery. 19th ed. Philadelphia, Pa: Elsevier Saunders; 2012. chap 52. Stephenson ER, Ilahi O, Koltun WA. Stoma creation through the stoma site: A rapid, safe technique. Dis Colon Rectum 1997;40:112-5. DOI: 10.1007/BF02055693 Mattingly M. Minimally invasive, endoscopically assisted colostomy can be performed without general anesthesia or laparotomy. Dis Colon Rectum 2003;46(2):271-3. DOI: 10.1007/s10350-004-6534-0 Senapati A, Phillips RKS. The trephine colostomy: A permanent left iliac fossa end colostomy without recourse to laparotomy. Ann R Coll Surg Engl 1991;305:305-6. Oliveira L, Reissman P, Nogueras J, et al. Laparoscopic creation of stomas. Surg Endosc 1997;11:19-23. DOI: 10.1007/s004649900287 Hellinger MD, Martínez SA, Parra-Davila E, et al. Gasless laparoscopic-assisted intestinal stoma creation through a single incision. Dis Colon Rectum 1999;42:1228-31. DOI: 10.1007/BF02238581 Patel P, Wright A, Messersmith R, et al. Does trephine colostomy produce a satisfactory stoma? Colorectal Dis 2001;3:270-1. Molina-Infante J, Mateos-Rodríguez JM, Vinagre-Rodríguez G, et al. Endoscopic-assisted colopexy and push percutaneous colostomy in the transverse colon for refractory chronic intestinal pseudo-obstruction. Surg Laparosc Endosc Percutan Tech 2011;21(6): e322-5. DOI: 10.1097/SLE.0b013e3182319a9e Cowlam S, Watson C, Elltringham M, et al. Percutaneous endoscopic colostomy of the left side of the colon. Gastrointest Endosc 2007;65(7):1007-14. DOI: 10.1016/j.gie.2007.01.012 Martin ST, Vogel JD. Intestinal stomas: Indications, management, and complications. Adv Surg 2012;46:19-49. DOI: 10.1016/j. yasu.2012.04.005 15. 16. 17. 18. 19. 20. 21. 22. 23. 24. Rev Esp Enferm Dig Sauer R, Becker H, Hohenberger W, et al. German Rectal Cancer Study Group. Preoperative versus postoperative chemoradiotherapy for rectal cancer. N Engl J Med 2004;351:1731-40. DOI: 10.1056/ NEJMoa040694 Kim JS, Hur H, Min BS, et al. Oncologic outcomes of self-expanding metallic stent insertion as a bridge to surgery in the management of leftsided colon cancer obstruction: Comparison with nonobstructing elective surgery. World J Surg 2009;33:1281-6. DOI: 10.1007/s00268-009-0007-5 Takahashi H, Okabayashi K, Tsuruta M, et al. Self-expanding metallic stents versus surgical intervention as palliative therapy for obstructive colorectal cancer: A meta-analysis. World J Surg 2015;39(8):2037-44. DOI: 10.1007/s00268-015-3068-7 Van Hooft JE, Van Halsema EE, Vanbiervliet G, et al. European Society of Gastrointestinal Endoscopy. Self-expandable metal stents for obstructing colonic and extracolonic cancer: European Society of Gastrointestinal Endoscopy (ESGE) Clinical Guideline. Endoscopy 2014;46(11):990-1053. DOI: 10.1055/s-0034-1390700 Imbulgoda A, MacLean A, Heine J, et al. Colonic perforation with intraluminal stents and bevacizumab in advanced colorectal cancer: Retrospective case series and literature review. Can J Surg 2015;58(3):167-71. DOI: 10.1503/cjs.013014 Carne PW, Robertson GM, Frizelle FA. Parastomal hernia. Br J Surg 2003;90:784-93. DOI: 10.1002/bjs.4220 Jugool S, McKain ES, Swarnkar K, et al. Laparoscopic or trephine faecal diversion: Is there a preferred approach and why. Colorectal Dis 2005;7:156-8. DOI: 10.1111/j.1463-1318.2004.00730.x Liu J, Bruch HP, Farke S, et al. Stoma formation for fecal diversion: A plea for the laparoscopic approach. Tech Coloproctol 2005;9:9-14. DOI: 10.1007/s10151-005-0185-6 Navarra G, Occhionorelli S, Marcello D, et al. Gasless video-assisted reversal of Hartmann’s procedure. Surg Endosc 1995;9:687-9. DOI: 10.1007/BF00187940 Nylund G, Oresland T, Hulten L. The trephine stoma: Formation of a stoma without laparotomy. Eur J Surg 1997;163:627-9. Caruso DM, Kassir AA, Robles RA, et al. Use of trephine stoma in sigmoid volvulus. Dis Colon Rectum 1996;39:1222-6. DOI: 10.1007/ BF02055112 Mukherjee A. Colonoscopy-assisted colostomy - An alternative to laparotomy: Report of two cases. Dis Colon Rectum 1998;41(11):145860. DOI: 10.1007/BF02237067 Parithivel VS, Schein M, Gerst PH. Colonoscopy-assisted “trephine” sigmoid colostomy. Dig Surg 2003;20(2):103-6. DOI: 10.1159/000069380 Patel JA, Fleshman JW, Hunt SR, et al. Is an elective diverting colostomy warranted in patients with an endoscopically obstructing rectal cancer before neoadjuvant chemotherapy? Dis Colon Rectum 2012;55:249-55. Rev Esp Enferm Dig 2017;109(4):273-278 PAPER Long-term results of subtotal colectomy for acquired hypertrophic megacolon in eight dogs OBJECTIVES: To evaluate the long-term results of subtotal colectomy for acquired hypertrophic megacolon in the dog. METHODS: Eight dogs with acquired hypertrophic megacolon underwent subtotal colectomy with preservation of the ileocolic junction. Long-term follow-up was obtained by clinical records and telephone interviews with the owners. RESULTS: Eight large-breed dogs (age range: 6 to 12 years; mean age: 10 75 years) were enrolled. The use of bone meal, low levels of exercise, chronic constipation with dyschesia and tenesmus refractory to medical management were factors predisposing dogs to acquired hypertrophic megacolon. The diagnosis was confirmed in all animals by abdominal palpation, plain radiography and postoperative histopathological findings. There were no intraoperative complications. One dog died as a result of septic peritonitis. The clinical conditions (that is, resolution of obstipation and stool consistency) of the remaining seven dogs were improved at discharge; all animals returned to normal defecation in five to 10 weeks (mean: 7 3 weeks) and were alive 11 to 48 months (mean: 40 5 months) after surgery. CLINICAL SIGNIFICANCE: Predominantly bony diet and/or low levels of physical activity may predispose dogs to acquired hypertrophic megacolon. Our results emphasise the long-term effectiveness of subtotal colectomy with preservation of the ileocolic junction in this condition. T. NEMETH, N. SOLYMOSI AND G. BALKA* Journal of Small Animal Practice (2008) 49, 618–624 DOI: 10.1111/j.1748-5827.2008.00624.x Department and Clinic of Surgery and Ophthalmology, *Department of Pathology and Forensic Veterinary Medicine, Faculty of Veterinary Science, Szent István University, Budapest, Hungary 618 INTRODUCTION Megacolon is characterised by the presence of an enlarged, hypomotile colon. This condition has been reported to occur in human beings (Swenson and Bill 1948), cats (Dietzmann 1968), dogs (Bright and others 1986) and pigs (Bassett and others 1999). In human beings, congenital megacolon (Hirschsprung’s disease) is caused by the failed migration of colonic ganglion cells during gestation. Varying lengths of the Journal of Small Animal Practice distal colon are unable to relax, causing functional colonic obstruction (Ehrenpreis 1970). Acquired megacolon may result from long-standing mechanical or functional bowel obstruction and may be classified as either primary or secondary. In cats, the causes and treatment of primary idiopathic megacolon have received considerable attention (Bright and others 1986, Rosin and others 1988, Bertoy and MacCoy 1989, Barreau 1994, Washabau and Hasler 1997, Washabau and Holt 1999). Specifically, it has been proposed that secondary megacolon can develop as a result of chronic obstructive lesions (for example pelvic canal stenosis) affecting the colon (Holt and Brockman 2003). Alternatively, this condition may be caused by neurological abnormalities resulting from sacral nerve injury or sacral spinal cord deformity (MacPhail 2002). Although canine-acquired megacolon has been described previously (Sahay and others 1983, Bright and others 1986, Barreau 1994, Petrus and others 2001), data concerning the long-term clinical outcome of this condition remain scanty. Nonetheless, medical (Hall and Washabau 1997, Hasler and Washabau 1997) and surgical strategies for the treatment of feline and canine megacolon have been described. Specifically, subtotal or total colectomy has been advocated as the treatment of choice in cases non-responsive to medical therapy (Fellenbaum 1978, Bright and others 1986, Bertoy and MacCoy 1989, De Haan and others 1992, Barreau 1994). In this case series, we sought to evaluate the long-term results of subtotal colectomy for acquired hypertrophic megacolon in the dog. We therefore reviewed the clinical data of eight dogs treated by this technique during a 5-year period. MATERIALS AND METHODS A total of eight dogs were included in the study. All animals had a history of bony diet, low levels of exercise, chronic Vol 49 December 2008 Ó 2008 British Small Animal Veterinary Association Colectomy for acquired hypertrophic megacolon in dogs constipation with dyschesia and tenesmus refractory to medical management performed by practitioners or veterinary internists before surgery. Medical management of constipation was attempted in all cases with oral stool softeners (paraffin oil or lactulose), prokinetics (sennoside and/or cisapride) and regular enemas (with warm water and oil). Despite thorough medical management, inability to defecate persisted in all dogs. Clinical examination revealed anorexia, significant weight loss, regular vomiting and a markedly distended abdomen with a palpable dilated intestine. Enlargement of the diameter of the colon beyond 1.5 times the length of the body of the seventh lumbar vertebra was shown by plain radiography in all dogs. Dogs suffering from other clinical conditions that could have lead to megacolon (for example, neurological disorders, stenosis of the pelvic canal, prostatic diseases and perineal hernia) were excluded from this study. Age, breed, sex, clinical signs (for example, general impression, circulatory and respiratory parameters, abdominal signs, tenesmus and constipation), duration of clinical signs, laboratory data (haematological and biochemical assessment), perioperative events and clinicopathological findings were recorded. Long-term follow-up was based (1) on the review of the clinical records and (2) on telephone interviews with the owners. All animals were parenterally treated with 10 mg/kg amoxicillin/clavulanic acid (Augmentin; Glaxo-SmithKline) plus 30 mg/kg enrofloxacin (Ganadexil Enrofloxacina; Invesa) for two days before surgery. Preoperative enemas were unsuccessful in all dogs. Premedication was achieved with 001 mg/kg iv acepromazine (Vetranquil; Ceva) and 005 mg/kg iv fentanyl (Fentanyl; Gedeon Richter) as a loading bolus followed by a constant-rate infusion of fentanyl. Intravenous 4 mg/kg propofol (Fresenius Propofol; Fresenius Kabi) was used for induction. Maintenance was achieved with a mixture of oxygen and isoflurane (Isoflurane USP; Phoenix Pharmaceutical) administered by inhalation. Following a lower ventral midline laparotomy, the intraoperative diagnosis of megacolon was established based on the presence of massive distension of the large bowel, which was filled with hard faecal masses. Manual removal of the faeces was attempted unsuccessfully in all cases. All dogs underwent subtotal colectomy with preservation of the ileocolic junction and caudal mesenteric arteries and veins. Intestinal transit was re-established with an end-to-end colocolic anastomosis using two layers (penetrating and Lembert) of simple interrupted sutures. A 3/0 USP absorbable monofilament suture material (polydioxanone, PDS) was used in all dogs. A passive abdominal Penrose drain was placed for three to four days. Postoperative analgesia was achieved by the continuation of constant-rate infusion with 005 mg/kg iv fentanyl (Fentanyl; Gedeon Richter) followed by a single injection of 02 mg/kg meloxicam (Metacam; Boehringer) once per day. Oral administration of a concentration diet (Concentration Diet, Waltham) was started on the first day after surgery, followed by canned soft food for three days. The drain was removed three to four days postoperatively. All dogs were successfully discharged five to seven days after surgery in improved clinical conditions. Owners were educated to feed animals with a moisturised soft diet and to enhance opportunities for physical activity. Antibiotic medications were discontinued one week after surgery. At the time of follow-up, owners were telephonically interviewed on the current clinical conditions of operated dogs, the features of defecation, the quality and quantity of stools. They were also asked their general opinion on the clinical management. The study variables (duration of tenesmus and constipation, time to normal defecation after surgery and survival rate) were statistically analysed in the R environment. Correlations between two variables were assessed with the Pearson’s correlation coefficient. RESULTS All dogs (age range: six to 12 years; mean age: 1025622 years, median: 11 years) with megacolon belonged to large breeds (for example Hungarian Kuvasz, Caucasian shepherd dog and German shepherd dog) (Table 1). The male to female ratio Table 1. General characteristics of dogs included in this study No. Signallment (breed, sex, age) History of tenesmus and constipation (weeks) Predominant clinical finding Anorexia, irregular vomiting, distended colon filled with hard faeces, obstipation Anorexia, abdomen painful and stiff on palpation, distended colon filled with bony faeces, obstipation, mild bloody peritoneal effusion Distended colon filled with hard faeces, obstipation Remarkable cachexia, anorexia and apathy, stiff and painful abdomen, distended colon filled with hard faeces, obstipation Anorexia, distended colon filled with hard faeces, obstipation, irregular bloody discharge from the anus Distended colon filled with hard faeces, obstipation Anorexia, distended colon and rectum filled with hard faeces, obstipation Distended colon filled with hard faeces, obstipation 1 Hungarian Kuvasz, male, 12 years 22 2 Caucasian shepherd dog, male, 9 years 24 3 4 Sarplaninac, male, 12 years English mastiff, male, 10 years 11 20 5 Mongrel, male, 9 years 26 6 7 German shepherd dog, male, 12 years Mongrel, female, 12 years 16 24 8 Caucasian shepherd dog, male, 6 years Journal of Small Animal Practice 5 Vol 49 December 2008 Ó 2008 British Small Animal Veterinary Association Time to Survival at Age at study follow-up normal (months) (years) faeces (weeks) 7 40 15.3 6 44 126 6 9 11 45 13 137 5 48 13 — 10 — 475 — 16 8 46 98 619 T. Nemeth and others was 7:1. The use of bone meal, low levels of exercise, chronic constipation (duration range: five to 26 weeks, mean 185673 weeks, median: 21 weeks) with dyschesia and tenesmus refractory to medical management were factors predisposing dogs to acquired hypertrophic megacolon. All animals underwent unsuccessful medical treatment for at least two months. No concurrent disease had been previously reported by the owners or the referring practitioners. The predominant clinical features were weight loss, anorexia and vomiting. A markedly distended abdomen with a palpable dilated intestine extending up to the epigastrium was present in all cases. Clinical laboratory abnormalities included mild anaemia, slightly elevated packed cell volume, and a mild leucocytosis with lymphopenia. Colonic distension with stool retention was evident on plain radiography (Fig 1). The spillage of bowel contents during surgery occurred in two cases (1 and 3) and dissection of the grossly distended colon was challenging (Fig 2). Moreover, requirements for sterility were not easily achieved during resection and anastomosis. Nonetheless, no intraoperative surgical complications occurred. Surgical suturing was easy to achieve by means of penetrating sutures placed into the thickened colonic wall. The excised colonic segments were submitted for histopathological evaluation. Several different stains (haematoxylineosin, Azan, Mallory trichrome and Van Gieson) were used. Histopathology revealed thickening of bowel wall because of the hypertrophy of smooth muscle cells, especially within the tunica muscularis and the lamina muscularis mucosae. Both the inner circular and outer longitudinal layers of smooth muscle were hypertrophic at histology. The muscle layers of the affected dogs’ colon were approximately twice as thick as the corresponding layers of the same colonic section from a healthy dog of the same size and bodyweight (Fig 3). The mucosa and lamina propria were intact in all cases, the only exception being dog 5. Specifically, in this case, there was inflammation and ulceration of the mucous membrane with infiltration of histiocytes and plasma cells. Dog 6 died on the fifth postoperative day, although microbiological examination in this dog revealed an Escherichia coli strain susceptible to amoxicillin/clavulanic acid and enrofloxacin used perioperatively. Necroscopy disclosed septic peritonitis without disruption of the anastomoses. The remaining seven dogs were discharged in improved clinical conditions. These dogs were all alive 11 to 48 months (mean: 405 months) after surgery according to the telephone interviews conducted with the owners. The return of normal defecation (two to three times a day, faeces of normal consistency) without tenesmus occurred between five and 10 weeks (mean: 73618 weeks, median: seven weeks) postoperatively. This process occurred with a gradual decrease in the frequency of daily defecation (from 10 to 12 daily episodes of moderate diarrhoea) alongside an increasing consistence of the faecal material (with two to three evacuations per day). Clinical management was judged to be satisfactory by all owners. A weak negative correlation was seen between age at time of surgery and survival at time of follow-up. No other significant correlations were detected. DISCUSSION FIG 1. Left lateral (A) and ventrodorsal (B) plain abdominal radiographs of the large intestine of dog 5. Distended colon filled with hard faecal material. Radiographic confirmation of megacolon was based on the comparison between the increase in colonic diameter (arrow marked with Dc) and the length of the seventh lumbar vertebra (arrow marked with L7LV) according to the O’Brien (1978) formula: Dc $ 15x L7LV 620 FIG 2. Intraoperative picture of megacolon during sceletisation (A). End-to-end colocolonic anastomosis with simple interrupted sutures (B) Journal of Small Animal Practice Congenital megacolon (also known as Hirschsprung’s disease in human beings) is caused by the absence of inhibitory neurons in Auerbach’s and Meissner’s plexuses (Garrett and others 1969) leading to spastic contraction of the affected segment with subsequent dilation of the proximal bowel section (Ehrenpreis 1970). Although the exact causes of megacolon in small animals have not been clearly identified yet, the absence of myenteric ganglia in the distal colon has been described in two cats (Yoder and others 1968, Ly 1977) and the occurrence of colon aganglionosis has been reported in two other cats (Rosin and others 1988). Acquired megacolon is generally idiopathic or secondary to neurogenic, Vol 49 December 2008 Ó 2008 British Small Animal Veterinary Association Colectomy for acquired hypertrophic megacolon in dogs FIG 3. Histology findings (40-fold magnification) in normal colon (upper row) and hypertrophic megacolon (lower row). Several different stains (haematoxylin-eosin, Azan, Mallory trichrome and Van Gieson) were used alimentary or orthopaedic causes. Most cases of feline megacolon are idiopathic, and the most common clinical symptoms include chronic anorexia, vomiting, weight loss, constipation and tenesmus (Bright and others 1986, Bertoy and MacCoy 1989, Barreau 1994, Washabau and Holt 1999, Holt and Brockman 2003). Although the exact aetiology of this condition remains to be elucidated, a primary neurological or degenerative neuromuscular cause has been suggested to play a role (Washabau and Stalis 1996). Although canine megacolon has been previously described in the literature, data regarding the clinical course and outcome in this condition are scarce. An 8-year-old entire male German shepherd dog with focal ulcerative colitis and megacolon has been described (Bright and others 1986). After unsuccessful attempts to evacuate the colon with multiple enemas, subtotal colectomy with removal of the ileocolic junction and end-to-side ileocolostomy was performed. The dog continued to show tenesmus despite excellent health and appetite five years after surgery. A 65year-old Lhasa Apso suffering from obstipation and megacolon because of bony diet has been also reported. Enterotomy and surgical removal of obstructing hard faeces were performed. Surgery was followed by laxative diet and proved to be successful Journal of Small Animal Practice (Sahay and others 1983). Moreover, a review paper has described three dogs with megacolon secondary to different primary conditions such as imperforate anus (in a one-month-old entire male boxer), postovariohysterectomy pelvic canal stenosis (in an eight-year-old neutered female Pincher) and cauda equina compression (in a 10year-old entire male German shepherd dog). The paper did not report the clinical course and outcomes of all dogs (Barreau 1994). A dog suffering from acquired dilated megacolon secondary to autonomic ganglioneuritis has also been reported (Petrus and others 2001). In this case, a four-year-old entire female Labrador retriever was treated unsuccessfully with enemas, lactulose and cisapride. The dog was then treated by surgical evacuation of the impacted colon through an incision. Unfortunately, constipation recurred after temporary improvement of constipation, and the owner refused subtotal colectomy. Thus the dog was euthanased. In the present case series, all dogs had a history of long-lasting constipation refractory to appropriate medical treatment with dietary interventions, laxatives (emollient oil and lactulose), prokinetics (sennoside or cisapride), and enemas. Calcium sennosides (designated A and B) are hydroxyanthracene glycosides derived from senna leaves. They have been used Vol 49 December 2008 Ó 2008 British Small Animal Veterinary Association as natural, safe, time-tested laxatives in both traditional and modern medicine. Although oral or intracolonic sennosides may inhibit myoelectric activity in the colon for 12 to 18 hours after a three to six hour delay, three to 10 contractions with a high amplitude (giant contractions) appear during the inhibition, thereby eliminating faecal matter and causing diarrhoea (Fioramonti and others 1988, Staumont and others 1988). Cisapride has been shown to stimulate smooth muscle contraction along the entire length of the colon (Hasler and Washabau 1997). Ranitidine and nizatidine, two H2-receptor antagonists, have also been shown to stimulate colonic peristalsis (Hall and Washabau 1997). The effect of mitemcinal (GM611), a novel orally active motilin agonist, on defecation has been investigated in rabbits and dogs. This compound has been shown to increase stool weight in a dosedependent fashion, without causing loose stools (Sudo and others 2007). Owners reported a predominantly bony diet in all dogs described in the present study. In this regard, the mechanical obstruction by firm ingesta may play a role in the weakening of bowel contractions. Nonetheless, in an experimental study in the dog, artificial distension of the ileum inhibited ileal motility and relaxed the colon as detected by barostat, thereby resulting in short-term dilation of the large bowel in the absence of mechanical obstruction. The resting tone of the colon was shown to be under adrenergic, cholinergic-nicotinic and nitric oxide-like-mediated inhibitory control; however, these agents cannot mediate solely the inhibition of the colonic tone elicited by ileal distension (Basilisco and Phillips 1994). Notably, all animals were kept in gardens on chains or in kennels without possibility of walks or exercise. The influence of regular physical activity on colonic transit time and defecation has been previously studied in middle-aged sedentary human patients suffering from chronic idiopathic constipation. Exercise resulted in a significant reduction in the percentage of incomplete defecation, the percentage of defecation requiring straining and the percentage of hard stools. The rectosigmoid and total colonic transit time similarly decreased, thereby suggesting that a lack 621 T. Nemeth and others of physical activity can lead to constipation in humans (De Schryver and others 2005). In keeping with these findings, the absence of physical activity may have contributed to bowel hypomotility and the development of constipation in our case series. The diagnosis of megacolon in our study was supported by typical physical findings including an extremely distended colon filled with hard faeces and extending up to the epigastrium. Notably, rectal digital palpation did not disclose any anomaly (for example pelvic canal stenosis) (Bertoy 2002). Radiographic examination showed pathognomonic signs of megacolon (that is dilated colonic sections filled with hard faeces). In our study, the radiological diagnosis of megacolon was confirmed when the enlargement of the diameter of the colon was beyond 15 times the length of the body of the seventh lumbar vertebra (O’Brien 1978). Alternatively, megacolon can be confirmed if the diameter of the colon exceeds the length of the body of the second lumbar vertebra (Lee and Leowijuk 1982). However, megacolon is a functional disease. Thus, the diagnosis is chiefly based on history, physical examination and confirmation of extremely distended bowel filled with hard faecal matter. In this regard, radiology findings may support the diagnosis. Several antibiotic regimens have been tested in colorectal surgery. A large review of randomised controlled trials of human antimicrobial prophylaxis did not show a clear superiority of one specific regimen; however, some inadequate regimens were identified (Song and Glenny 1998). Broad-spectrum activity against both Gram-positive and Gram-negative aerobic and anaerobic isolates is essential in this setting (Holt and Brockman 2003, Niles and Williams 2005). This could be achieved by amoxicillin and clavulanic acid, but this combination is ineffective against Enterobacter and Pseudomonas (Graber 1998). Because of its activity against these bacteria, enrofloxacin may offer a valuable option (Plumb 1999). Antibiotics were administered during the attempts to evacuate the colon. As the rich bacterial population, the high intraluminal pressure and the prolonged lag phase of colon healing may increase the risk of dehiscence for at least four days postoperatively (Niles and 622 Williams 2005), the continuation of the perioperative antibiotic administration may have exerted beneficial effects. In the present study, preoperative enemas were not attempted because several previous conservative efforts had failed. Furthermore, routine use of enemas before colotomy or colectomy remains controversial. Indeed, there is evidence to suggest that it could be associated with an increased risk of leakage and gross abdominal contamination (Bertoy 2002, Niles and Williams 2005). This could be ascribed to the change of dry, hard and easily manipulated faeces into an infectious liquid milieu (Holt and Brockman 2003). However, mechanical cleaning remains the standard practice before elective colonic resection in human beings (Nichols and others 1997). Although manual removal of faeces from the colonic segment to be resected is recommended (Holt and Brockman 2003), the removal of solid faeces from the resection sites was difficult in our study. Thus far, several surgical techniques for the management of megacolon have been described, mainly in cats. In this regard, previous techniques such as coloplasty with the reduction of the diameter of the affected bowel (Bruce 1959), and partial colectomy with removal of a segment of the affected colon alongside with the ileocolic junction and the caecum (Yoder and others 1968) are no longer performed. In the present study, we performed a subtotal colectomy with preservation of the ileocolic junction and the caudal mesenteric artery and vein, followed by the creation of an end-to-end colocolic anastomosis. The ileocolic junction was preserved, inasmuch as it minimises the development of postoperative diarrhoea because of bacterial overgrowth (Bright and others 1986, Holt and Johnston, 1991). Preservation of the caudal mesenteric artery and vein is beneficial because it maximises blood supply to the remaining distal colonic segment (Washabau and Holt 1999). However, there is little evidence that surgical closure of the caudal mesenteric vessels would significantly impair the blood supply of the caudal colonic segment and the rectum. A number of techniques have been reported as for the restoration of bowel continuity after subtotal colectomy, including end-to-end, end-to-side and sideJournal of Small Animal Practice to-side colocolostomies (Barreau 1994, White 2002). In a study the recovery from diarrhoea after subtotal colectomy occurred at eight postoperative weeks. The recovery was confirmed by the return of a normal bowel transit time, decreased moisture volume, and reconstruction of cholinergic fibres in the anastomotic section (Jimba and others 2002). Several experimental studies aiming to evaluate the clinical outcomes of total colectomy followed by ileoproctostomy or ileoanal anastomosis in the dog have shown that persistent diarrhoea, skin excoriation and nocturnal incontinence occur in the majority of cases (Mibu and others 1987, Ferrara and others 1992). This is in contrast to the cases reported in this manuscript. It is possible that the resolution of diarrhoea and return of normal consistency stools in this case series reflects the less radical surgery performed with preservation of both the ileocolic junction, colorectal junction and rectum. This complication may be overcome via different interventions. Specifically, the use of an antiperistaltic ileal segment can maintain solid stools, normal weight and electrolyte and water balance (Tuley and others 1976). Interposition of a jejunal segment into the anorectal area may increase absorption of water, sodium and chloride from the operated intestinal section (Mibu and others 1987). Preservation of faecal continence may be achieved by application of an ileal (J-) pouch as a functionally passive reservoir after proctocolectomy (Sarmiento and others 1997, Willis and others 2004, 2007). The potential utility of total/complete colectomy with resection of the ileocolic junction has been also suggested, producing an ileocolic or ileorectal anastomosis (Fellenbaum 1978, Bright and others 1986, Bertoy and MacCoy 1989). In our study, a double layer (penetrating and seromuscular) simple interrupted pattern with 3/0 USP absorbable monofilament suture material (polydioxanone, PDS) was used for anastomosis in all dogs according to papers reporting that appropriate anastomosis can be achieved by a two-layer closure (Bright and others 1986, Barreau 1994, White 2002). However, a single-layer simple interrupted pattern with polydioxanone suture material has mostly been recommended for large Vol 49 December 2008 Ó 2008 British Small Animal Veterinary Association Colectomy for acquired hypertrophic megacolon in dogs intestinal anastomoses in cats (De Haan and others 1992, Sweet and others 1994, Bertoy 2002, MacPhail 2002, Holt and Brockman 2003). The use of a simple continuous suture pattern after subtotal colectomy has also been reported (Bright and others 1986) and may not have significant disadvantages compared with the simple interrupted technique (Pavletic and Berg 1996). In our study, no clinical evidence of stenosis or disruption was seen when a handsawn double layer (penetrating and Lembert) of simple interrupted sutures was used. In this context, the extremely increased diameter of the colon may prevent the two-layer technique from causing a remarkable stricture. Although one dog (no. 6) died of diffuse septic peritonitis on the fifth postoperative day, suture insufficiency was not seen at necropsy. The surgical stapling technique to create a circular two-layer inverting end-to-end anastomosis (EEA device) has also been described (Kudisch and Pavletic 1993, Kudisch 1994, MacPhail 2002, Holt and Brockman 2003). Alternatively, a biofragmentable intestinal anastomosis ring may also be used for large intestinal anastomoses, by placing a specific ring (875 per cent polyglyconic acid plus 125 per cent barium sulphate) between the two cut ends (Barreau 1994, Huss and others 1994). In our study, histopathological evaluation revealed prominent smooth muscle hypertrophy in the affected colon, as confirmed by the presence of massively thickened muscle layers. Histological data in acquired megacolon affecting small animals – especially in the dog – are scarce. The main histopathological features of idiopathic megacolon in cats are minor abnormalities in smooth muscle cells or in myenteric and submucosal neurons (Washabau and Stalis 1996). The presence of mucosal alterations (ulceration and inflammatory cell infiltration) chiefly depends on the duration of the process and is affected by the type and amount of ingesta and the bacterial population. In a previous study, colonic biopsies of four cats undergoing subtotal colectomy because of idiopathic megacolon revealed mucosal fibrosis with diffuse, chronic mild colitis, severe submucosal congestion and focal chronic ulcerative colitis with compensatory muscle hyperplasia (Bright and Journal of Small Animal Practice others 1986). A human study reviewing 894 cases of megacolon disclosed the presence of mucosal ulcers, mucosal hyperplasia and chronic inflammation (Garcia and others 2003). Altered contractile proteins and neural innervation in idiopathic megarectum and megacolon were reported in another human study (Gattuso and others 1998). Aberrant innervation because of traumas or autonomic ganglioneuritis may result in megacolon in the dog (Petrus and others 2001). In such cases, the tunica muscularis of the affected area is either normal or thinner, respectively. In the present study, smooth muscle hypertrophy is likely to act as a compensatory mechanism elicited by an increased resistance to hard ingesta (fecalith) in the absence of underlying neurogenic or orthopaedic diseases. Nevertheless, the contribution of lowgrade chronic obstructive disease to the development of megacolon cannot entirely be ruled out. Although the major causes of acute postoperative complications such as infection, haemorrhage, ischaemia or obstruction (Barreau 1994) did not occur in our study, one dog died of septic peritonitis. Notably, the microbiological examination revealed E. coli contamination. The strain was sensitive to amoxicillin and clavulanic acid. As during surgery for megacolon a massive bacterial invasion of the operating site may occur, postoperative drainage can be considered (Holt and Brockman 2003). No definite data on time, indication and methods for abdominal drainage are currently available even in colorectal surgery in human beings. Human surgeons generally use abdominal lavage and drains as a second stage procedure when anastomosis leakage or peritonitis occur (Faranda and others 2000, Chouillard and others 2007). It should be noted, however, that the effectiveness of intraoperative drainage have been questioned (Merad and others 1998, Yeh and others 2005). The therapeutic efficacy and complications of abdominal drainage in canine colorectal surgery has not been adequately addressed. In any case, we have no clear evidence that the drain may exert beneficial effects by preventing septic complications. Nevertheless, the possibility of ascending contamination through the abdominal drain cannot be ruled out. Vol 49 December 2008 Ó 2008 British Small Animal Veterinary Association The remaining seven dogs were discharged in improved clinical conditions and defecating liquid stools six to eight times a day. According to the results of telephone interviews with the owners, the long-term effectiveness of subtotal colectomy with preservation of the ileocolic junction in canine megacolon seems promising. Normal or nearly normal defecation (passage of faeces of normal consistency two to three times a day) was achieved within five to 10 weeks. No complications similar to those reported in cats – recurrence of constipation, weight loss, constant diarrhoea, tenesmus or rectal bleeding (White 2002) – were seen in this study. In a previous study, the enteric function of four cats undergoing subtotal colectomy for megacolon was compared with that of four normal cats. Cats treated surgically were healthy and thriving and, in general, enteric function was similar to that of controls. Bowel movements occurred only slightly more frequently, with no significant differences in faecal volume or water content. The results of this study did not provide evidence of an abnormal subclinical bowel function occurring in cats after subtotal colectomy (Gregory and others 1990). These data are in keeping with our present findings. Accordingly, in our study all dogs regained good physical conditions, and all are still alive at a mean of 405 months after surgery. In conclusion, this study suggests that an exclusively bony diet in combination with low levels of physical activity may predispose dogs to acquired hypertrophic megacolon. Our results emphasise the long-term effectiveness of subtotal colectomy with preservation of the ileocolic junction in this condition. References BARREAU, P. (1994) Mégacolon chez le chien et le chat. Pratique Medical et Chirurgical de l’Animal de Compagnie 29, 721-729 BASILISCO, G. & PHILLIPS, S. F. (1994) Ileal distention relaxes the canine colon: a model of megacolon? Gastroenterology 106, 606-614 BASSETT, J. R., MANN, F. A., CONSTANTINESCU, G. M. & MCCLURE, R. C. (1999) Subtotal colectomy and ileocolic anastomosis in a Vietnamese pot-bellied pig with idiopathic megacolon. Journal of the American Veterinary Medical Association 215, 1640-1642 BERTOY, R. W. (2002) Megacolon in the cat. The Veterinary Clinics Small Animal Practice 32, 901-915 BERTOY, R. W. & MACCOY, D. M. (1989) Total colectomy with ileorectal anastomosis in the cat. Veterinary Surgery 18, 204-210 623 T. Nemeth and others BRIGHT, R. M., BURROWS, C. F., GORING, R., FOX, S. & TILTMANT, L. (1986) Subtotal colectomy for treatment of acquired megacolon in the dog and cat. Journal of the American Veterinary Medical Association 188, 1412-1416 BRUCE, R. H. (1959) Operation for megacolon in cats. Modern Veterinary Practice 40, 66 CHOUILLARD, E., MAGGIORI, L., ATA, T., JARBAOUI, S., RIVKINE, E., BENHAIM, L., GHILES, E., ETIENNE, J. C. & FINGERHUT, A. (2007) Laparoscopic two-stage left colonic resection for patients with peritonitis caused by acute diverticulitis. Diseases of the Colon and Rectum 50, 1157-1163 DE HAAN, J. J., ELLISON, G. W. & BELLAH, J. R. (1992) Surgical correction of idiopathic megacolon in cats. Feline Practice 20, 6-11 DE SCHRYVER, A. M., KEULEMANS, Y. C., PETERS, H. P., AKKERMANS, L. M., SMOUT, A. J., DE VRIES, W. R. & BERGE-HENEGOUWEN, G. P. (2005) Effects of regular physical activity on defecation pattern in middleaged patients complaining of chronic constipation. Scandinavian Journal of Gastroenterology 40, 422-429 DIETZMANN, U. (1968) Occurrence of the congenital megacolon (Hirschsprung’s mega-colon) in cats. Monatshefte für Veterinärmedizin 23, 349-352 EHRENPREIS, T. (1970) Hirschsprung’s Disease. Chicago, IL, USA: Year Book FARANDA, C., BARRAT, C., CATHELINE, J. M. & CHAMPAULT, G. G. (2000) Two-stage laparoscopic management of generalized peritonitis due to perforated sigmoid diverticula: eighteen cases. Surgical Laparoscopy, Endoscopy & Percutaneous Techniques 10, 135-138 FELLENBAUM, S. (1978) Partial colectomy in the treatment of recurrent obstipation/megacolon in the cat. Veterinary Medicine/Small Animal Clinician 73, 737-742 FERRARA, A., PEMBERTON, J. H. & HANSON, R. B. (1992) Preservation of continence after ileoanal anastomosis by the coordination of ileal pouch and anal canal motor activity. American Journal of Surgery 163, 83-89 FIORAMONTI, J., STAUMONT, G., GARCIA-VILLAR, R. & BUENO, L. (1988) Effect of sennosides on colon motility in dogs. Pharmacology 36, 23-30 GARCIA, S. B., ARANHA, A. L., GARCIA, F. R., BASILE, F. V., PINTO, A. P., DE OLIVEIRA, E. C. & ZUCOLOTO, S. (2003) A retrospective study of histopathological findings in 894 cases of megacolon: what is the relationship between megacolon and colonic cancer? Revista do Instituto de Medicina Tropical de São Paulo 45, 91-93 GARRETT, J. R., HOWARD, E. R. & NIXON, H. H. (1969) Autonomic nerves in the rectum and colon in Hirschsprung’s disease. Archives of Disease in Childhood 44, 406-417 GATTUSO, J. M., SMITH, V. V. & KAMM, M. A. (1998) Altered contractile proteins and neural innervation in idiopathic megarectum and megacolon. Histopathology 33, 34-38 GRABER, H. (1998) Antimicribás kemoterápia. In: Gyógyszertan. Ed ZS. Fürst. Medicina, Budapest, Hungary. pp 858-920 GREGORY, C. R., GUILFORD, W. G., BERRY, C. R., OLSEN, J. & PEDERSON, N. C. (1990) Enteric function in cats after subtotal colectomy for treatment of megacolon. Veterinary Surgery 19, 216-220 HALL, J. A. & WASHABAU, R. J. (1997) Gastrointestinal prokinetic therapy: acetylcholinesterase inhibitors. Compendium on Continuing Education for the Practicing Veterinarian 19, 615-620 624 HASLER, A. H. & WASHABAU, R. J. (1997) Cisapride stimulates contraction of idiopathic megacolonic smooth muscle in cats. Journal of Veterinary Internal Medicine 11, 313-318 HOLT, D. E. & BROCKMAN, D. (2003) Large intestine. In: Textbook of Small Animal Surgery. Ed D. H. Slatter. Saunders, Philadelphia, PA, USA. pp 665-682 HOLT, D. & JOHNSTON, D. E. (1991) Idiopathic megacolon in cats. Compendium on Continuing Education for the Practicing Veterinarian 13, 1411-1416 HUSS, B. T., PAYNE, J. T. & JOHNSON, G. C. (1994) Comparison of a biofragmentable intestinal anastomosis ring with appositional suturing for subtotal colectomy in cats. Veterinary Surgery 23, 466474 JIMBA, Y., NAGAO, J. & SUMIYAMA, Y. (2002) Changes in gastrointestinal motility after subtotal colectomy in dogs. Surgery Today 32, 1048-1057 KUDISCH, M. (1994) Surgical stapling of large intestines. Veterinary Clinics of North America: Small Animal Practice 24, 323-333 KUDISCH, M. & PAVLETIC, M. M. (1993) Subtotal colectomy with surgical stapling instruments via a trans-cecal approach for treatment of acquired megacolon in cats. Veterinary Surgery 22, 457463 LEE, R. & LEOWIJUK, C. (1982) Normal parameters in abdominal radiology of the dog and cat. Journal of Small Animal Practice 23, 251-269 LY, J. T. (1977) Surgical correction of megacolon in a cat. Australian Veterinary Practice 7, 210-212 MACPHAIL, C. (2002) Gastrointestinal obstruction. Clinical Techniques in Small Animal Practice 17, 178-183 MERAD, F., YAHCHOUCHI, E., HAY, J. M., FINGERHUT, A., LABORDE, Y. & LANGLOIS-ZANTAIN, O. (1998) Prophylactic abdominal drainage after elective colonic resection and suprapromontory anastomosis: a multicenter study controlled by randomization. French Associations for Surgical Research. Archives of Surgery 133, 309-314 MIBU, R., ITOH, H. & NAKAYAMA, F. (1987) Effect of total colectomy and mucosal proctectomy on intestinal absorptive capacity in dogs. Diseases of the Colon and Rectum 30, 47-51 NICHOLS, R. L., SMITH, J. W., GARCIA, R. Y., WATERMAN, R. S. & HOLMES, J. W. (1997) Current practices of preoperative bowel preparation among North American colorectal surgeons. Clinical Infectious Diseases 24, 609-619 NILES, J. D. & WILLIAMS, J. M. (2005) The large intestine and rectum. In: Bsava Manual of Canine and Feline Abdominal Surgery. Eds J. M. Williams and J. D. Niles. Bsava, Gloucester, UK. pp 125-140 O’BRIEN, T. R. (1978) Large Intestine. In: Radiographic Diagnosis of Abdominal Disorders in the Dog and Cat. Ed T. R. O’Brien. W. B. Saunders, Philadelphia, PA, USA. pp 352-395 PAVLETIC, M. M. & BERG, J. (1996) Gastrointestinal surgery. In: Complications in Small Animal Surgery. Eds A. J. Lipowitz, D. D. Caywood, C. D. Newton and A. Schwartz. Williams & Wilkins, Baltimore, MD, USA. pp 365-389 PETRUS, D. J., NICHOLLS, P. K. & GREGORY, S. P. (2001) Megacolon secondary to autonomic ganglioneuritis in a dog. The Veterinary Record 148, 276-277 PLUMB, D. C. (1999) Veterinary Drug Handbook. Iowa State University Press, Ames, IA, USA ROSIN, E., WALSHAW, R., WEHLHAFF, C., MATTHIESEN, D., ORSHER, R. & KUSBA, J. (1988) Subtotal colectomy for treatment of chronic constipation associated Journal of Small Animal Practice with idiopathic megacolon in cats: 38 cases (1979–1985). Journal of American Veterinary Medical Association 193, 850-853 SAHAY, P. N., KHAN, A. A., DEOKIOULIYAR, U. K. & DASS, L. L. (1983) Obstipation and megacolon in a dog. Modern VeterinaryPractice 64, 130-131 SARMIENTO, J. M., PEMBERTON, J. H. & REILLY, W. T. (1997) Physiologic determinants of nocturnal incontinence after ileal pouch-anal anastomosis. Journal of Gastrointestinal Surgery 1, 324-330 SONG, F. & GLENNY, A. M. (1998) Antimicrobial prophylaxis in colorectal surgery: a systematic review of randomized controlled trials. British Journal of Surgery 85, 1232-1241 STAUMONT, G., FIORAMONTI, J., FREXINOS, J. & BUENO, L. (1988) Changes in colonic motility induced by sennosides in dogs: evidence of a prostaglandin mediation. Gut 29, 1180-1187 SUDO, H., OZAKI, K., MURAMATSU, H., KAMEI, K., YOGO, K., CYNSHI, O., KOGA, H., OMURA, S. & TAKANASHI, H. (2007) Mitemcinal (GM-611), an orally active motilin agonist, facilitates defecation in rabbits and dogs without causing loose stools. Neurogastroenterology and Motility 19, 318-326 SWEET, D. C., HARDIE, E. M. & STONE, E. A. (1994) Preservation versus excision of the ileocolic junction during colectomy for megacolon: a study of 22 cats. Journal of Small Animal Practice 35, 358-363 SWENSON, O. & BILL, A. H. Jr (1948) Resection of rectum and rectosigmoid with preservation of the sphincter for benign spastic lesions producing megacolon. Surgery 24, 212-218 TULEY, R. D., MATOLO, N. M., GARFINKLE, S. E. & WOLFMAN, E. F.Jr (1976) Antiperistaltic bowel segment for prevention of ileoproctostomy diarrhea. Journal of Surgical Oncology 8, 67-73 WASHABAU, R. J. & HASLER, A. H. (1997) Constipation, obstipation, and megacolon. In: Consultations in Feline Internal Medicine. 3rd edn. Ed J. R. August. Saunders, Philadelphia, PA, USA. pp 104-112 WASHABAU, R. J. & HOLT, D. (1999) Pathogenesis, diagnosis and therapy of feline idiopathic megacolon. Veterinary Clinics of North America: Small Animal Practice 29, 589-603 WASHABAU, R. J. & STALIS, I. H. (1996) Alterations of colonic smooth muscle functions in cats with megacolon. American Journal of Veterinary Research 57, 580-587 WHITE, R. N. (2002) Surgical management of constipation. Journal of Feline Medicine and Surgery 4, 129-138 WILLIS, S., HÖLTZ, F., WEIN, B., VON FELBERT, V., FACKELDEY, V. & SCHUMPELICK, V. (2004) Defecation mechanisms after proctocolectomy and ileal pouch-anal anastomosis in dogs. International Journal of Colorectal Diseases 19, 228-233 WILLIS, S., HÖLTZ, F., WEIN, B. & SCHUMPELICK, V. (2007) Defecation mechanisms after anterior resection J-pouch-anal and side-to-end anastomosis in dogs. International Journal of Colorectal Diseases 22, 161-165 YEH, C. Y., CHANGCHIEN, C. R., WANG, J. Y., CHEN, J. S., CHEN, H. H., CHIANG, J. M. & TANG, R. (2005) Pelvic drainage and other risk factors for leakage after elective anterior resection in rectal cancer patients: a prospective study of 978 patients. Annals of Surgery 241, 9-13 YODER, J. T., DRAGSTEDT, L. R. & STARCH, C. J. (1968) Partial colectomy for correction of megacolon in a cat. Veterinary Medicine, Small Animal Clinician 63, 1049-1052 Vol 49 December 2008 Ó 2008 British Small Animal Veterinary Association