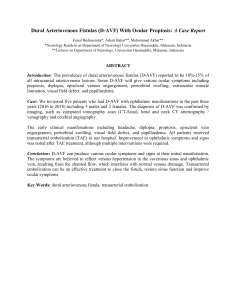
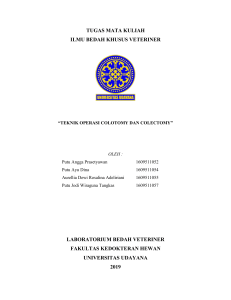
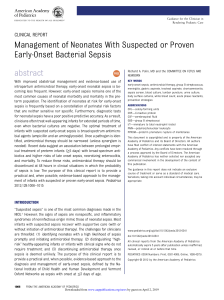
[Downloaded free from http://www.hamdanjournal.org on Friday, May 15, 2020, IP: 10.232.74.27] Review Article Current Concepts in the Management of Anorectal Malformations Carlos A. Reck‑Burneo Department of Pediatric Surgery, Medical University of Vienna, Vienna, Austria Abstract Anorectal malformations (ARMs) occur in approximately 1 of every 5000 newborns and management still differs widely among practitioners. In this review, we address some of the currently accepted concepts in management. Mismanagement can have devastating consequences such as fecal incontinence, urinary incontinence, and sexual dysfunction. We briefly review common peculiarities of the most common cases the and initial management of the newborn. I intend to present a brief overview without going into details but to motivate interest and further reading in this topic. Further, the recommendation is made that case referral to a center with the expertise and ideally a high volume case load, which provides the highest benefits for the patient. Keywords: Anorectal malformations, congenital illnesses, incontinence Introduction Anorectal malformations (ARMs) occur in approximately 1 of every 5000 newborns.[1] That represents around 1.5 million babies born each year worldwide with this condition. This number is an extrapolation that probably underrepresents the actual incidence. The most common sequelae, when not treated properly, are faecal incontinence, urinary incontinence and sexual disfucntion.[2] As a consequence, social isolation can lead to depression and mental health issues. ARMs, unfortunately, rank highly amongst mistreated and/or undertreated congenital illnesses. Here, we present an overview and essential management pearls. Newborn Baby with Anorectal Malformation In the first days of life and after neonatal stabilising interventions are in place, it is essential to rule out comorbidities. Screening for the whole spectrum of the vertebral defects, anal atresia, cardiac defects, tracheoesophageal fistula, renal anomalies and limb abnormalities association (VACTERL) is paramount and should not be delayed.[2,4‑6] After careful perineal examination, a prone cross table X‑ray after the 24 h of life can help to establish the type of Access this article online Quick Response Code: Website: www.hamdanjournal.org malformation first by showing air in the rectum.[7] No decision as to the correct management should be performed before the first 24 h of life as the colonic intraluminal pressure would not suffice to expel meconium through a small fistula.[1] An abdominal ultrasound should be performed to evaluate for hydronephrosis and in a female for hydrocolpos [Figure 1].[6,8,9] Sacrospinal defects occur in 30% of patients, and even though this does not merit critical evaluation, it will have a significant impact on establishing functional prognosis. The quality of the sacrum and the presence of a tethered cord or presacral mass are essential and in combination with the original diagnosis will help us evaluate the potential for continence. Therefore, a sacral X‑ray and evaluation of the spinal cord either by ultrasound or a magnetic resonance imaging are necessary.[1,10] Finally, the decision needs to be made towards the necessity of a colostomy. Colostomy Depending on the type of malformation, a colostomy will allow decompression of the intestine, protection of a repaired Address for correspondence: Dr. Carlos A. Reck‑Burneo, Department of Pediatric Surgery, Medical University of Vienna, Währinger Gürtel 18‑20, 1190 Vienna, Austria. E‑mail: [email protected] This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms. For reprints contact: [email protected] DOI: 10.4103/HMJ.HMJ_66_18 100 How to cite this article: Reck‑Burneo CA. Current concepts in the management of anorectal malformations. Hamdan Med J 2018;11:100-4. © 2018 Hamdan Medical Journal | Published by Wolters Kluwer - Medknow [Downloaded free from http://www.hamdanjournal.org on Friday, May 15, 2020, IP: 10.232.74.27] Reck-Burneo: Basic concepts in the management of ARM’s Figure 1: Correct way to examine an anorectal malformation in females Figure 2: Positioning of the child for the correction of an anorectal malformation Figure 3: 3D reconstruction of a cloacal malformation Figure 4: Cloacal malformation perineum, renal protection from recurrent urinary tract infections and allow performing a distal colostogram to establish the appropiate diagnosis. Children born in centres where no dedicated paediatric surgical department exists, or if; the surgeons do not have enough experience treating ARMs; it is recommended to perform a colostomy and refer the child to a specialised centre. The colostomy is still the safest way to manage children with ARM and should always be used in cases of doubt. Furthermore, in cases where the rectal air bubble seems to be above the coccyx, a colostomy will allow for a distal colostogram. When perfroming a colsotomy please consider that this surgical procedure also carries high morbidity and also has peculiarities described elsewhere.[11] Moreover, in developing countries, colostomy care can be challenging and this can lead to skin affections and irritation. The accepted consensus is to do a colostomy with separated stomas in the first mobile portion of the descending colon as to avoid prolapse and to prevent stool from entering the urinary tract.[12] Hamdan Medical Journal ¦ Volume 11 ¦ Issue 3 ¦ July-September 2018 Anorectal Malformation Types and Clinical Approach In 2005, the Krickenbeck classification was introduced as a more precise tool to classify and diagnose ARM, thus allowing better prognostic and therapeutic prediction of the underlying problem.[13] [Table 1] The details of each diagnosis are beyond the scope of this review, and for a more detailed explanation, we suggest reading a paediatric surgical textbook [Figure 2]. I do want to emphasise some key concepts and will detail some of those here. Female Rectovestibular fistula The most common female anorectal malformation is a fistula located in the vestibule, outside the hymen and often erroneously labelled as a rectovaginal fistula.[14] In experienced hands, this defect can be operated primarily and does not require a colostomy.[15,16] Decompression and emptying of 101 [Downloaded free from http://www.hamdanjournal.org on Friday, May 15, 2020, IP: 10.232.74.27] Reck-Burneo: Basic concepts in the management of ARM’s Table 1: Krickenbeck classification of anorectal malformations Major clinical groups Perineal (cutaneous) fistula Rectourethral fistula Prostatic bulbar Rectovesical fistula Vestibular fistula Cloaca ARM with no fistula Anal stenosis ARM: Anorectal malformations Rare variants Pouch colon atresia/stenosis Rectal atresia/stenosis Rectovaginal fistula H‑type fistula others meconium are through the fistula, and in some cases, dilations can be considered to bridge to definitive surgery.[1] As a rule of thumb, if there are three perineal orifices in a female, the diagnosis is a perineal fistula or a vestibular fistula. In both cases, primary repair is to be considered, and the long‑term prognosis is good given a normal sacrum and a normal spinal cord with no pre‑sacral mass.[9,17,18] Cloaca A single perineal orifice in the place a normal urethra would be located, is by definition a cloaca, given the absence of an anus Figures 2 and 4. [19] This is the third most common female anorectal malformation and in many cases misdiagnosed.[20,21] The variations and classification are out of the scope of this review, and further reading is recommended. [22] In a cloaca, a colostomy should be performed. Urological abnormalities are frequent with this abnormality and urological emergencies need to be addressed.[8] Thus, a full urological evaluation is necessary after birth or as soon as possible. If an hydrocolpos is present, it needs to be permanently drained at the time of the colostomy creation. The surgical care of the cloaca should be referred to a specialised centre with experience treating it. Its complexity can range from mild cases with a short common channel to complex cases that have a long common channel.[23] The treatment option varies depending on the length of the urethra and the common channel. Management includes total urogenital mobilisation for milder cases with a short channel and a complete dissection of the vagina from the urethra in cases with a long channel. In many cases, a colonic interposition is required to make up for a missing or short vagina.[24] Extensive post‑operative care and long‑term management are essential on top of a good technical operation by an experienced surgeon.[24,25] Males Perineal fistula This is the lowest of all defects in males and it can mislead the surgeon into believing that correction is simple. The anterior wall is usually fused to the urethra, and urethral injury is possible.[1] When technically well performed, good continence can be expected. This defect can be repaired by primary repair in experienced hands. If not, the fistula can 102 be dilated to allow for appropriate meconium emptying and the repair delayed for 2–3 months. It is essential to allow complete bowel emptying through the fistula as otherwise a megarectum will complicate the procedure and worsen the prognosis.[26] The most common complication as in most ARM will be constipation and post‑operative bowel management, especially in the initial years will ensure an excellent prognosis later.[27] Rectourethral fistula This is the most common anorectal malformation in males. The rectum can connect to the urethra in any part of its trajectory, but it is most commonly connected to the bulbous urethra and in worst cases to the prostate.[9] For this type of malformation, an initial colostomy is recommended to prevent contamination of the urinary tract and to allow a proper diagnosis in the form of a distal colostogram is essential. In cases of a prostatic fistula, an abdominal or laparoscopic approach may be necessary preceding the posterior sagittal anorectoplasty.[28] The potential for continence will also be given in part by the baseline diagnosis on top of the quality of the sacrum and spinal cord. Prostatic fistulas often show an anteriorly located muscle complex and in many cases have a decreased buttock crease which has a poor prognosis for continence. In many of these cases, bowe management to achieve social incontinence is often required for the whole life of the individium.[29] Bladder neck fistula This is the defect with the worst prognosis in males. A colostomy should always be performed when suspected. In this group, laparoscopy is helpful as a pelvic approach may not allow to reach the rectum. Laparoscopy will also facilitate separation of the rectum from the bladder. Even though no common wall exists between the bladder and the rectum, both structures can be tightly attached and separation is difficult, especially when the attachment is prolonged beyond the fistulous tract. In some cases where the entry of the fistula is perpendicular to the bladder, laparoscopy is especially suited and the separation easy to perform. The outcome of bladder neck fistulas is commonly faecal incontinence, and when the surgery is poorly performed, there is a high risk of urinary incontinence.[30] Anal dilations Recommendations are changing with regard to anal dilations with studies currently looking at the exact indication for them. previous management stated to start dilations at 2–4 weeks after the procedure, and this still applies to most cases. Parents have to learn to do it by themselves. In some centres, weekly dilations in the hospital are preferred to daily parental dilations allowing for sedation and better pain therapy to prevent trauma. Functional sequela The most common sequela is constipation, and it is utterly vital to aggressively treat it to avoid a mega rectosigmoid. [31] Undertreated constipation will lead to Hamdan Medical Journal ¦ Volume 11 ¦ Issue 3 ¦ July-September 2018 [Downloaded free from http://www.hamdanjournal.org on Friday, May 15, 2020, IP: 10.232.74.27] Reck-Burneo: Basic concepts in the management of ARM’s incontinence and overflow pseudoincontinence. This needs to be aggresively treate to prevent persisten incontinence. Urinary incontinence is also frequent especially in cloacas and bladder neck fistulas. An abdominal X‑ray can help to diagnose impaction and then stimulant laxatives should be given titrating to the best dose‑effect amount.[32] Patients that by 3 years of age are not continent or clean require aggressive bowel management. In this systematic programme, parents and patients are instructed on how to keep the colon empty with either laxatives or an enema programme.[31] 7. 8. 9. 10. 11. 12. 13. Conclusion In this review, we have addressed some of the current concepts in the management of ARM. New ideas that have gained traction and are currently being explored are the long‑term outcomes with an emphasis on quality of life. New concepts such as the health literacy, quality of life and psychosocial aspects of ARM are still early in research and will contribute to the management of this chronic ailment.[33‑35] Great strides are made in the surgical and operative aspects but other areas require prompt attention and care. Centralisation is now commonly accepted as the road to better outcomes in rare diseases. It improves care and with ith the quality of life in patients with ARM’s. Only a centre with enough volume can offer enough experience to the surgical trainee and attending and will have enough volume to allow a multidisciplinary care and most of all appropriate follow‑up and correct bowel management. A more oftenly seen challenge is transition to adult care as adult surgeons barely know about the lifelong implications that ARM can have. Research opportunities in this field are extensive and will hopefully be addressed by a new generation of paediatric surgeons in this field. Financial support and sponsorship Nil. 14. 15. 16. 17. 18. 19. 20. 21. 22. 23. 24. Conflicts of interest There are no conflicts of interest. 25. References 26. 1. 2. 3. 4. 5. 6. Wood RJ, Levitt MA. Anorectal malformations. Clin Colon Rectal Surg 2018;31:61‑70. Shaul DB, Harrison EA. Classification of anorectal malformations – Initial approach, diagnostic tests, and colostomy. Semin Pediatr Surg 1997;6:187‑95. Minneci PC, Kabre RS, Mak GZ, Halleran DR, Cooper JN, Afrazi A, et al. Screening practices and associated anomalies in infants with anorectal malformations: Results from the Midwest pediatric surgery consortium. J Pediatr Surg 2018;53:1163‑7. Lane VA, Ambeba E, Chisolm DJ, Lodwick D, Levitt MA, Wood RJ, et al. Low vertebral ano‑rectal cardiac tracheo‑esophageal renal limb screening rates in children with anorectal malformations. J Surg Res 2016;203:398‑406. Totonelli G, Catania VD, Morini F, Fusaro F, Mosiello G, Iacobelli BD, et al. VACTERL association in anorectal malformation: Effect on the outcome. Pediatr Surg Int 2015;31:805‑8. Belman AB, King LR. Urinary tract abnormalities associated with imperforate anus. J Urol 1972;108:823‑4. Hamdan Medical Journal ¦ Volume 11 ¦ Issue 3 ¦ July-September 2018 27. 28. 29. 30. 31. Reck‑Burneo CA, Vilanova‑Sanchez A, Wood RJ, Levitt MA, Bates DG. Imaging in anorectal and cloacal malformations. Pediatr Radiol 2018;48:443‑4. Levitt MA, Bischoff A, Peña A. Pitfalls and challenges of cloaca repair: How to reduce the need for reoperations. J Pediatr Surg 2011;46:1250‑5. Peña A. Anorectal malformations. Semin Pediatr Surg 1995;4:35‑47. Bui CJ, Tubbs RS, Oakes WJ. Tethered cord syndrome in children: A review. Neurosurg Focus 2007;23:E2. Bischoff A, Levitt MA, Lawal TA, Peña A. Colostomy closure: How to avoid complications. Pediatr Surg Int 2010;26:1087‑92. Bischoff A, Levitt MA, Peña A. Update on the management of anorectal malformations. Pediatr Surg Int 2013;29:899‑904. Holschneider A, Hutson J, Peña A, Beket E, Chatterjee S, Coran A, et al. Preliminary report on the international conference for the development of standards for the treatment of anorectal malformations. J Pediatr Surg 2005;40:1521‑6. Levitt MA, Bischoff A, Breech L, Peña A. Rectovestibular fistula – Rarely recognized associated gynecologic anomalies. J Pediatr Surg 2009;44:1261‑7. Moore TC. Advantages of performing the sagittal anoplasty operation for imperforate anus at birth. J Pediatr Surg 1990;25:276‑7. Menon P, Rao KL. Primary anorectoplasty in females with common anorectal malformations without colostomy. J Pediatr Surg 2007;42:1103‑6. Arnoldi R, Macchini F, Gentilino V, Farris G, Morandi A, Brisighelli G, et al. Anorectal malformations with good prognosis: Variables affecting the functional outcome. J Pediatr Surg 2014;49:1232‑6. Kyrklund K, Pakarinen MP, Koivusalo A, Rintala RJ. Bowel functional outcomes in females with perineal or vestibular fistula treated with anterior sagittal anorectoplasty: Controlled results into adulthood. Dis Colon Rectum 2015;58:97‑103. Levitt MA, Peña A. Cloacal malformations: Lessons learned from 490 cases. Semin Pediatr Surg 2010;19:128‑38. Levitt MA, Peña A. Anorectal malformations. Orphanet J Rare Dis 2007;2:33. Rosen NG, Hong AR, Soffer SZ, Rodriguez G, Peña A. Rectovaginal fistula: A common diagnostic error with significant consequences in girls with anorectal malformations. J Pediatr Surg 2002;37:961‑5. Peña A. Cloaca – Historical aspects and terminology. Semin Pediatr Surg 2016;25:62‑5. Rintala RJ. Congenital cloaca: Long‑term follow‑up results with emphasis on outcomes beyond childhood. Semin Pediatr Surg 2016;25:112‑6. Wood RJ, Reck‑Burneo CA, Dajusta D, Ching C, Jayanthi R, Bates DG, et al. Cloaca reconstruction: A new algorithm which considers the role of urethral length in determining surgical planning. J Pediatr Surg 2017. pii: S0022‑3468(17)30644‑9. Vilanova‑Sanchez A, Reck CA, McCracken KA, Lane VA, Gasior AC, Wood RJ, et al. Gynecologic anatomic abnormalities following anorectal malformations repair. J Pediatr Surg 2018;53:698‑703. Kyrklund K, Pakarinen MP, Taskinen S, Rintala RJ. Bowel function and lower urinary tract symptoms in males with low anorectal malformations: An update of controlled, long‑term outcomes. Int J Colorectal Dis 2015;30:221‑8. Rintala RJ. Congenital anorectal malformations: Anything new? J Pediatr Gastroenterol Nutr 2009;48 Suppl 2:S79‑82. Shawyer AC, Livingston MH, Cook DJ, Braga LH. Laparoscopic versus open repair of recto‑bladderneck and recto‑prostatic anorectal malformations: A systematic review and meta‑analysis. Pediatr Surg Int 2015;31:17‑30. Kyrklund K, Pakarinen MP, Koivusalo A, Rintala RJ. Long‑term bowel functional outcomes in rectourethral fistula treated with PSARP: Controlled results after 4‑29 years of follow‑up: A single‑institution, cross‑sectional study. J Pediatr Surg 2014;49:1635‑42. Hassett S, Snell S, Hughes‑Thomas A, Holmes K 10‑year outcome of children born with anorectal malformation, treated by posterior sagittal anorectoplasty, assessed according to the Krickenbeck classification. J Pediatr Surg 2009;44:399‑403. Bischoff A, Levitt MA, Peña A. Bowel management for the treatment of 103 [Downloaded free from http://www.hamdanjournal.org on Friday, May 15, 2020, IP: 10.232.74.27] Reck-Burneo: Basic concepts in the management of ARM’s pediatric fecal incontinence. Pediatr Surg Int 2009;25:1027‑42. 32. Vilanova‑Sanchez A, Gasior AC, Toocheck N, Weaver L, Wood RJ, Reck CA, et al. Are senna based laxatives safe when used as long term treatment for constipation in children? J Pediatr Surg 2018;53:722‑7. 33. Dingemans AJ, Reck CA, Vilanova‑Sanchez A, Gonzalez DO, Gasior AC, Weaver LJ, et al. Does clinic visit education within a multidisciplinary center improve health literacy scores in caregivers of children with complex colorectal conditions? J Pediatr Surg 104 2017;52:1997‑2000. 34. Grano C, Bucci S, Aminoff D, Lucidi F, Violani C. Quality of life in children and adolescents with anorectal malformation. Pediatr Surg Int 2013;29:925‑30. 35. Clermidi P, Podevin G, Crétolle C, Sarnacki S, Hardouin JB. The challenge of measuring quality of life in children with Hirschsprung’s disease or anorectal malformation. J Pediatr Surg 2013;48:2118‑27. Hamdan Medical Journal ¦ Volume 11 ¦ Issue 3 ¦ July-September 2018