ARTICLE
Developmental
Kathleen
FOCUS
E. Gilbride,
Testing
PhD*
QUESTIONS
1. What
role do developmental
screening
tests have in the monitoring
of growth
and development
in pediatric
practice?
2. What
precautions
must be taken
in the interpretation
of the results
of developmental
screening
tests
for individual
children?
3. How do the reliability,
validity,
sensitivity,
and specificity
of developmental
tests affect the interpretation
of their results?
4. What
developmental
screening
and full-scale
developmental
tests
are available?
What are their
strengths
and weaknesses?
Development
during
infancy
and
childhood
is a dynamic
process
that
generally
unfolds
in a predictable
sequence.
The age at which
specific
milestones
are achieved
may vary
within
a given range,
with spurts and
lags in development
occurring
commonly.
Parents
frequently
turn to pediatricians
when questions
and concerns about their child’s
development
arise. The pediatrician
can help the
parents
determine
whether
their child
is experiencing
a temporary
lag in a
specific
area (eg, late walking),
a
more serious
developmental
delay or
disability
(eg, retardation
or cerebral
palsy),
or a significant
behavioral
problem
(eg, hyperactivity,
school
failure).
The pediatrician
can use ongoing developmental
surveillance
to
monitor
a child’s
progress,
with developmental
screening
and testing
as
supplementary
tools to screen
for and
diagnose
problems,
initiate
early intervention,
and design
appropriate
treatment.
Developmental
Surveillance
Developmental
surveillance
refers to
an ongoing
process
of monitoring
a
child’s
developmental
status at each
pediatric
visit and includes
taking
a
thorough
history,
reviewing
developmental
milestones,
making
skilled
Assistant
Professor
of Pediatrics,
University
of California at Los Angeles,
Harbor-UCLA
Medical
Center,
Torrance,
CA.
338
observations
of the child, and eliciting parental
concerns.’
This process
provides
an understanding
over time
of that child’s
developmental
trajectory. It allows
the pediatrician
to observe the child’s
rate of development,
temperamental
style, and emotional
adj ustment
to developmental
phases
(eg, separation,
independence).
In
addition,
the pediatrician
learns about
the parents’
knowledge
and attitudes
about parenting
and the nature
of the
parent-child interaction. This is particularly
important
information
because it provides
the backdrop
against
which future
interpretations
and decisions
about the child’s
behavior
and development
will be
made.
Developmental
surveillance
also helps the pediatrician
to build a
trusting
relationship
with the parent,
which
is critical
in the event that delays or difficulties
arise that require
intervention.
Parents
who believe
that
the pediatrician
knows
their child
well are more likely to work with the
pediatrician
when intervention
is
needed.
Developmental
Screening
During
the course
of developmental
surveillance,
screening
tests can be
used to assess the child’s
developmental
status periodically.
These
tests
are meant
to be brief, easily administered measures
designed
to assess
the
child’s
current
developmental
functioning
globally
compared
with a
standardized
sample
of children
of
the same age. The purpose
of such
tools is to identify children who have
delays
(which
would
mean that it has
high sensitivity),
while accurately
classifying
others
who do not have
delays
(which
would
indicate
that it
has high specificity).
Although
developmental
screening
tests are too time-consuming
to be
included
at every health
care visit or
with every child followed,
using
them at key ages (eg, 6, 9, 12, and
18 months
and 2, 3, 4, and 5 years)
is a useful
way of monitoring
the
achievement
of developmental
milestones,
especially
with children
at
increased
risk of delay.
In fact, re-
peated
measures
are needed
to form
an accurate
picture
of the child’s
developmental
progression
because
occasional
lags are common
in normal
development.
A single
measure
at a
given time may be confounded
by
several
factors
(eg, fatigue,
illness,
and lack of cooperation),
whereas
multiple
measures
will yield more
reliable results.
Developmental
screening
also provides parents
with periodic
feedback
about their child’s
progress
and opportunities
to discuss
developmental
concerns.
Parents
may lack knowledge of child development;
the developmental
screening
tool can be used
to educate
them about the normal
progression
of development.
This can
be especially
helpful
with parents
who have inappropriate
developmental expectations
for their child or for
those parents
who are anxious
about
their child’s
mastery
of deve]opmental tasks. Screening
tests can educate
the pediatrician
as well because
subjective
impressions
often can be maccurate.
By using screening
tools systematically,
the physician
increases
his or her knowledge
of normal
child
development
and experience
with
developmental
stages,
which
can, in
turn, improve
the identification
of
delays.
Periodic
developmental
screening
that aids in the early
detection
of
delays
is particularly
relevant
since
the passage
of Public
Laws 99-142
and 99-457.
PL 99-142
requires
states
to provide
an appropriate
education
to all school-age
children
regardless
of handicapping
condition; PL 99-457
requires
the states
to extend
these
services
to children
3 to 5 years
of age who are referred
with developmental
disabilities
and
to provide
early
intervention
to infants and toddlers
who are at increased
risk of having
developmental delays.
Infants
or children
of preschool
age who have disabilities
most likely
will be identified by pediatricians
because
they are not yet in the education
system.
Periodic
developmental screening
can help the pediatrician
to identify
delays
early, allowing
par-
Pediatrics in Review
Vol. 16
No. 9
Downloaded from http://pedsinreview.aappublications.org/ at University of Connecticut on May 26, 2015
September
1995
.
CHILD DEVELOPMENT
Developmental
Testing
,
than any other screening
instrument
in the field. Reliability
studies
have
shown
this tool to have high interrater reliability
(ie, consistency
across
raters)
and test-retest
reliability
(ie,
consistency
over short periods
of
time).
In terms
of validity,
the DDST
has been useful
in identifying
global
delay
and mental
retardation,
but children
who have mild developmental
delays
or speech
and Ianguage
difficulties
often
were not
identified.
As a result,
it has been
criticized
for its limited
predictive
validity
and low sensitivity,
that is,
it identified
some,
but not all children who had delays.
The restandardized
DDST
II is improved
in
this respect,
with greater
sensitivity
(ie, it classifies
a higher
percent
of
children
as being
at risk for delays),
but it appears
to have lower
specificity (ie, it is less accurate
in identifying
children
who do not have
ents to gain access
to intervention
services
as early as possible.
DENVER
SCREENING
DEVELOPMENTAL
TEST
II
The most common
screening
measured
used by pediatricians
is the
Denver
Developmental
Screening
Test (DDST),
which
recently
has
been
restandardized
as the DDST
11.2 The restandardization
was based
on a sample
of 2096 children
in the
Denver
area who were stratified
by
age, race, socioeconomic
status,
and
residential
area. It is designed
for
ages 2 weeks
to 6 years
and consists of 125 items
grouped
into four
areas:
Personal-Social,
Fine MotorAdaptive,
Language,
and Gross
Motor. It can be administered
easily
and scored
in 15 to 20 minutes.
Items
are scored
as either
passed
or
failed,
and profile
scores
are interpreted
as being
normal,
questionable, abnormal,
or untestable
in accordance
with the number
of passes
in each of the four areas.
No separate scores
are given
for each area.
The DDST
has been a successful
screening
instrument
because
of its
easy-to-use
format
and practical
use
in both clinical
and research
settings.
In addition
to the DDST
II, the
Revised-Denver
Prescreening
Developmental
Questionnaire
(R-DPDQ)
is available.
It is a checklist
of 97
items drawn
from the DDST
and can
be completed
by parents
in about
10 minutes.
Items are arranged
in
chronologic
order based on the ages
at which
90% of the standardization
sample
were able to perform
an item.
It has been suggested
as a first step
in the screening
process
to determine
areas of concern,
with follow-up
with
the DDST
if either two delays
are
evident
on initial screening
or one
delay persists
on two separate
occasions.
Screening
tests, however,
like all
psychometric
measures,
have limitations of which
the clinician
should
be
aware.
Most importantly,
the reliability and validity
of a screening
instrument should
be known.
Because
little
information
is available
about the
reliability
and validity
of the R-PDQ,
it should
be used very cautiously.
The DDST
and the DDST
II have
been researched
more extensively
Pediatrics in Review
Vol. /6
No. 9
tool to identify
risk, with
made
for more
extensive
assessment
when
indicated.
OTHER
DEVELOPMENTAL
SCREENING
TOOLS
Other
screening
measures
that appear to have high levels
of sensitivity, specificity,
reliability,
and validity
include
the Minnesota
Child
Development
Inventory
(MCDI)
and the Battelle
Developmental
Inventory
Screening
Test.3’4
The MCDI
consists
of 320 empirically
derived
questions
about development
and behavior
that are grouped
into seven
scales:
Gross
Motor,
Fine Motor,
Expressive
Language,
ComprehensionConceptual,
Situation
Comprehension, Self-Help,
and Personal-Social.
A General
Development
Scale is
composed
of items from the other
seven
scales.
It is designed
for children ages I to 6 years and can be
The DDST
is used better as a measure
of early
than as an assessment
of school-age
functioning.
delays).
As a result,
it has a higher
percentage
of false-positives
or
children
who do not have delays
but who are identified
as being
at
risk. This also lowers
its predictive
validity
in terms
of ability
to predict future
outcome.
Other
potential
problems
with the
DDST
II are common
for many
developmental
screening
instruments.
For example,
several
items
are
based
on parental
report
and not on
direct
observations.
If a parent
is an
unreliable
reporter,
the outcome
will have poor reliability.
At the
younger
age levels,
few items
are
related
to later functioning;
thus, it
is used best as a measure
of current
developmental
functioning
rather
than as a measure
to predict
later
outcome.
At the older
age levels,
a
limited
number
of items
are relevant to school
functioning,
yet clinicians
may use it to predict
school
functioning
or school
readiness.
It
probably
is used better
as a measure of early
development
than as
an assessment
of school-age
functioning.
Finally,
as with all screening instruments,
it should
not be
used for diagnosis,
but rather
as a
September
referrals
diagnostic
development
completed
by the parent
in
30 minutes.
Scores
are categorized
as
either
normal,
‘delayed,
or
Severely
delayed.’
with age levels provided for each scale.
The MCDI
has high sensitivity
and specificity;
however,
because
it
is based
on parental
report,
it is
subject
to some of the same
limitations
in reliability
and validity
as
the DDST.
Its major
drawback
is
the standardization
sample
on
which
the norms
are based.
The
standardization
sample
comprised
796 middle-class
Caucasian
children from Bloomington,
Minnesota.
The lack of diversity
in terms
of
race, geographic
region,
and socioeconomic
status
limits
its generalizability
to children
who do not fit
this demographic
profile.
The Battelle
is designed
for children 6 months
to 8 years old and
takes
10 to 30 minutes
to administer,
depending
on the child’s
age. It consists of 96 items taken from the 341
items in the full battery,
which
fall
into the categories
of Adaptive,
Motor, Cognitive,
Communication,
and
Personal-Social
skills.
Raw scores
are
converted
into T-scores
(mean
=
50,
‘ ‘
‘ ‘
‘
‘ ‘
‘ ‘
‘
1995
Downloaded from http://pedsinreview.aappublications.org/ at University of Connecticut on May 26, 2015
339
CHILD DEVELOPMENT
Developmental
Testing
standard
deviation
=
10) or Deviation Quotients
(mean
=
100, standard
deviation
=
15), and guidelines
for
referral
are given based on subtest
scores.
The standardization
sample
of
800 children
is based
on 1981 US
census
data stratified
by race, sex,
and geographic
region,
with a middIe-class
emphasis.
It has high testretest and interrater
reliability,
although
like other screening
measures,
some items depend
on parental
report, which will influence
its reliability. Validity
data indicate
high concurrence
with other standardized
measures,
and it differentiates
clinical
from nonclinical
samples,
with high
sensitivity
and specificity.
Predictive
validity
is limited
at the younger
age
levels,
as with most other screening
tools.
The Early Screening
children
4 to 6 years
of failing
in school.
Inventory
old who
Several
other screening
measures
are available
to identify
specific
areas
of functioning.
For example,
the
Clinical
Linguistic
and Auditory
Milestone
Scale (CLAMS)
and the
Early Language
Milestone
Scale
(ELMS)
are designed
for screening
language
development,
the Home
Screening
Questionnaire
(HSQ)
can
be used to identify
high-risk
factors
in the home,
and the Pediatric
Symptom Checklist
provides
a way of
screening
for behavioral
or emotional
problems.5
These
tools are useful
when the pediatrician
wants to screen
for a particular
area of developmental
functioning.
SCHOOL
READINESS
SCREENING
In addition
to the previously
mentioned
screening
tests,
the pediatrician should
be familiar
with school
readiness
screening
tests.
School
readiness
tests differ
from developmental
screening
tests by focusing
on a narrow
range
of abilities
that
are specific
to kindergarten
or first
grade.
Typically,
they include
cognitive,
language,
and fine motor
tasks as well as observations
of the
child’s
attention
span and social
skills
(eg, ability
to attend,
cooperate, and follow
directions).
They
are not designed
to provide
a diag340
nostic
evaluation
of the child’s
developmental
functioning.
Parents
may ask the pediatrician
to assess
whether
their child has the specific
skills
needed
to begin
school
or
they may approach
the pediatrician
after the school
has assessed
their
child’s
readiness.
Understanding
what readiness
tests are designed
to
do and not to do is essential
to
helping
the family
make appropriate
decisions
regarding
school
placement.
Because
school
readiness
tests
are intended
to measure
preparedness for academic
achievement,
their best purpose
is for instructional
planning
to identify
areas
that should
be addressed
in the kindergarten
curriculum
(such
as learning letters,
letter-sound
combina-
is designed
to identify
are at increased
risk
tions,
numbers).
Most children
who
have severe
delays
will have been
identified
before
school
entrance,
so
these
tests screen
for milder
problems that affect
school
performance.
Some
schools
use these
instruments
inappropriately
as admission
or diagnostic
tests to delay
the start of
school
or to keep a child
in kindergarten
a second
year. A low score
on a readiness
screening
test may
be interpreted
by the school
as mdicating
that the child
is immature
and schooling
should
be delayed
1 year, when,
in fact, school
enrollment may be exactly
what the child
needs,
with placement
in an educational
setting
that is appropriate
for
his or her learning
difficulties.
In
such cases
the pediatrician
can advocate
for a thorough
evaluation
because
decisions
about
placement
should
not be based
solely
on the
results
of a single
readiness
test.
This is especially
true given
that
many
readiness
tests have significant limitations
in reliability,
validity, standardization
sample,
and the
purpose
for which
they were designed.
A thorough
assessment
for school
readiness
should
include
a review
of
the medical
history,
a physical
examination
with a brief neurologic
screening,
and a vision
and hearing
Pediatrics
screening.
In addition,
a screening
test that is specific
to the skills required
in the school
should
be used
rather than a global
developmental
screening
tool. For example,
the
Early Screening
Inventory
(ES!) is
designed
specifically
to identify
children 4 to 6 years old who are at increased
risk for failing
in school.
failure. It assesses
abilities
related
to a
child’s
potential
for acquiring
knowledge rather than just his or her current skill achievement.
The ESI is administered
individually in 15 to 20 minutes,
with a
total score based
on items
computed
in three sections:
VisualMotor/Adaptive,
Language
and
Cognition,
and Gross
Motor/Body
Awareness.
Recommendations
are
provided
based
on the total score
and fall into one of three categories: 1) “OK”
for scores
that range
within
1 standard
deviation
of the
mean;
2) “Rescreen”
for scores
from
1 to 2 standard
deviations
below the mean,
with rescreening
recommended
in 8 to 10 weeks;
and
3) “Refer”
for scores
2 or more
standard
deviations
below
the mean,
with referral
for diagnostic
testing.
The ES! has been shown
to have
high test-retest
and interrater
reliability.
It has satisfactory
validity
when compared
with concurrent
measures,
and long-term
validity
(through
third grade)
has been
shown
to be high because
it identifled the majority
of children
accurately
who presented
later having
learning
problems.
Thus,
it has
high sensitivity,
with appropriate
specificity
as well. The ES! was
standardized
on 465 primarily
Caucasian
children
from low to lowermiddle
class urban
homes.
Therefore, it may be limited
in its
applicability
to other
samples
that
have different
racial,
socioeconomic
status,
or geographic
characteristics.
SUMMARY
Many
screening
tools are available
to
the pediatrician;
the ones described
here are just a sample
of some that
are used commonly.
Understanding
the purpose
and limitations
of each
screening
measure,
in terms of reliability,
validity,
sensitivity,
specificity, and the population
for which
it
was designed,
will help the pediatriin Review
Vol.
16
No.
Downloaded from http://pedsinreview.aappublications.org/ at University of Connecticut on May 26, 2015
9
September
1995
CHILD DEVELOPMENT
Developmental
Testing
cian use these tools effectively
to
identify
children
at risk for developmental
delay.
Most importantly,
the
pediatrician
should
view screening
tests as one source
of information
to
be used in an overall
strategy
of developmental
surveillance
that includes
careful
historical
review,
systematic
clinical
observations,
and
solicitation
of parental
concerns
and
attitudes.
Developmental
Testing
Once
the pediatrician
identifies
a
delay
or suspects
a developmental
problem,
the child
should
be referred
for formal
developmental
assessment.
Such
a referral
should
be discussed
with the parents
by
inquiring
first whether
they have
similar
concerns
regarding
their
child’s
development.
Many
parents
will have voiced
these
concerns
already,
or if they haven’t,
they
may have been silently
worried
that
something
was wrong
and readily
agree
to pursue
developmental
assessment.
It can be explained
to
parents
that a more extensive
developmental
assessment
can clarify
the
child’s
strengths
and weaknesses
and identify
areas
that would
benefit from
additional
stimulation
or
early
intervention.
The pediatrician
should
emphasize
that a single
developmental
assessment
does not
determine
a child’s
diagnosis
or
long-term
prognosis;
rather,
it provides
more
information
about
the
child’s current status, which the
pediatrician and parents can use in
deciding
about
appropriate
intervention. Most developmental
assessments
are conducted
best by a developmental
or child psychologist,
a
“developmental”
pediatrician,
or
other
professional
person
who has
received
special
training
in the
evaluation
of young
children.
DEVELOPMENTAL
TESTS
The most psychometrically
sound
instruments
for developmental
testing
are the Bayley
Scales
of Infant
Development
and its recent
revision,
the Bayley
II. ‘#{176}
The Bayley
was
designed
for children
ages 2 to
30 months and was standardized on
1262 infants
stratified
by age, geographic
area, gender,
race, and educaPediatrics
in Review
Vol.
16
No.
9
September
tion of parent.
It takes approximately
45 to 60 minutes
to administer
and
requires
a high level of training.
The
Bayley
II extends
the age range coyered to 1 to 42 months
and was restandardized
on I 700 children
who
were stratified
according
to age, gender, race/ethnicity,
geographic
region,
and parent
education,
based on 1988
US census
data. New items were
added,
and some items were modified
or deleted.
Both versions
of the Bayley
are
well-standardized
measures
that
consist
of a Mental
Scale,
a Psychomotor
Scale,
and an Infant
Behavior
Record
(referred
to as the
Behavior
Rating
Scale
on the Bayley II). Standardized
scores
that
have a mean
of I 00 and a standard
deviation
of 16 (15 for the Bayley
II) are produced
for the Mental
and
whereas
after 2 years
of age. language
becomes
very important
for
predicting
future
outcome.
The
Bayley
does not correlate
highly
with later measures
of intelligence
because
those
measures
emphasize
language
and abstract
reasoning.
Accordingly,
the Bayley
(or any
developmental
measure)
is used
best as a measure
of current
developmental
functioning,
rather
than as
a predictor
of later functioning.
To
monitor
the developmental
progress
of a child
who is delayed
or at increased
risk of being
delayed,
the
child
should
be assessed
repeatedly
over time. This is especially
true
for children
who receive
intervention, so that the effects
of the intervention
can be assessed
over time.
The Gesell
Developmental
Schedules was one of the earliest
stan-
The Bayley
Scales
of Infant
Development
for children
ages 2 to 30 months.
The
this age from
1 to 42 months.
Psychomotor
Scales.
The Infant
Behavior
Record
of the original
Bayley describes
the child’s
behavioral
style during
the evaluation,
including social
orientation,
cooperation,
fearfulness,
tension,
emotional
tone,
object
orientation,
goal directedness, attention
span, endurance,
activity,
and reactivity.
This scale
was revised
completely
in the
Bayley
II to provide
a systematic
5-point
scoring
system
for all items,
with the goal of facilitating
scoring
and interpretation
and improving
reliability.
An additional feature of the Bayley II is the inclusion
of four facets
(Cognitive, Language,
Personal/
Social,
and Motor
Quality)
designed
to help interpret
performance
on the
Mental
and Motor
Scales.
Items
on
both scales
are grouped
into one of
the facets
(based
on item-facet
correlations),
with a developmental
age
calculated
for each facet.
This allows one to look at the profile
of
strengths
and weaknesses
within
the
Mental and Motor Scales.
The Bayley
has very good reliability,
but limited
predictive
validity until a child
is 24 to 30 months
of age. Among
children younger
than 24 months,
development
primarily
is sensorimotor-based,
were designed
Bayley
II extends
dardized
measures
of infant
development
and was restandardized
in
1980 as the Revised
Gesell
and
Amatruda
Developmental
and Neurologic
Examination.’’
This test is
administered
in about
30 minutes
and is applicable
to infants
from
I
week
to 42 months
of age. Items
are categorized
into Adaptive,
Gross
Motor,
Fine Motor,
Language,
and Personal-Social
skills.
A
developmental
age is calculated
for
each category,
with a developmental quotient
calculated
based
on the
developmental
age achieved,
divided
by the chronological
age, and
multiplied
by 100. The Gesell
provides
useful
clinical
information;
however,
the standardization
is limited because
there
are few standardized instructions
and no standardized scores,
it is based
on small
normative
samples,
and there are
few data regarding
reliability
and
validity.
Psychological
Testing
Psychological
tests such as intelligence
tests, achievement
tests, or behavior
rating scales
should
be used
for preschool
to school-age
children
who have developmental
disabilities,
learning
difficulties,
or behavioral or
1995
Downloaded from http://pedsinreview.aappublications.org/ at University of Connecticut on May 26, 2015
34/
CHILD DEVELOPMENT
Developmental
Testing
emotional
problems.
A comprehensive assessment
battery
administered
by a child
psychologist
generally is most useful
for diagnosing
problems
in this age range
because
several
factors
often
interact
to produce learning
or behavior
difficulties. The child’s
or adolescent’s
intellectual
abilities,
academic
skills,
and behavioral
functioning,
as well as the family
context,
contribute
to any difficulty
that the pediatrician
may be asked
to address.
Typical
problems
in this age range
about
which
parents
ask pediatricians
include
learning
disabilities,
school
failure,
hyperactivity
or attention
deficit
disorders,
and behavior and emotional
disturbances.
Any assessment
battery
should
include a measure
of intellectual
functioning
to indicate
overall
cognitive
ability.
There are several
tests of intelligence;
the most widely
used ones
probably
are the Wechsler
scales.
These
include
the Wechsler
Preschool
and Primary
Scale of Intelligence-Revised
(WPPSI-R)
for children 3 years to 7 years,
3 months
old; the Wechsler Intelligence Scale
for Children III (WISC
III) for those
6 to 16 years; and the Wechsler
Adult Intelligence
Scale-Revised
(WAIS-R)
for those 16 years to
adulthood.’2’4
All of these measures
are well-standardized
and have wellestablished
reliability
and validity
(primarily
for predicting
school
performance).
Each test consists
of a
Verbal Scale and a Performance
(or
nonverbal)
Scale, with subtests
within
each domain that measure a variety
of skills.
Each subtest
provides
a
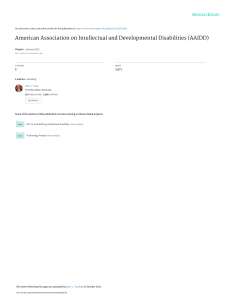
TABLE.
IQ RANGE
130 and
of IQ
Ranges
CLASSIFICATION
above
Very
superior
120-129
Superior
110-119
High
average
90-109
Average
80-89
Low
70-79
Borderline
69 and
Adapted
342
Classification
scaled
score (mean
=
I 0, standard
deviation
=
3); these
are combined
to produce
a Verbal
Intelligence
Quotient
(VIQ),
a Performance
IQ
(PIQ),
and a Full Scale
IQ (FSIQ).
The IQ scores
are standardized
based
on comparisons
with scores
earned
by same-age
peers
in the
standardization
group.
They
are
based
on a mean of 100 and a standard deviation
of 15 and allow
comparisons
across
ages. Thus,
an
average
IQ score
at any age is 100,
with the range
of 85 to 1 15 falling
within
I standard
deviation
of the
mean.
The Table
indicates
the range
of IQs and the diagnostic
category
assigned
to each.
The WISC
III often is used in an
assessment
battery
to assess
a child
for learning
problems.
The profile
of
subtest
scores
in the Verbal
and Performance
areas and the discrepancy
between VIQ and PIQ often are more
useful
in determining
the nature
of
cognitive
difficulties
than is the FSIQ.
For example,
a child who achieves
an
average FSIQ of 100, but who has a
significant
discrepancy
between
VIQ
and PIQ (eg, 90 versus
110) can be
described
as having
average
intelligence
but also a significant
difference
between
his or her verbal
and nonverbal
processing
abilities.
Analysis
of the child’s
profile
of scores
within
the Verbal
and Performance
areas
will identify
areas of strength
and
weakness
and suggest
areas in need
of remediation.
The Verbal Scale is comprised of
six subtests
(Information,
Similarities,
Arithmetic,
Vocabulary,
Comprehension, Digit Span) that depend
on the
below
from
Average
Mentally
Wechsler
(1991).
Deficient
child’s
receptive
and expressive
language
skills
and reflect
accumulated knowledge
and experience.
A
child’s
performance
on several
of
these
subtests
is influenced
by
school
experience,
including
the
Information,
Arithmetic,
and Vocabulary
subtests.
Other
subtests,
such as Comprehension
and Similarities,
require
knowledge
regarding social
norms
and comprehension of abstract
verbal
concepts,
respectively.
These
tasks are likely
to be influenced
by social
stimulation or deprivation.
Attention
and
concentration
also are required
for
successful
completion
of the Digit
Span and Arithmetic
subtests,
which
reflect
short-term
memory
skills.
The Performance
Scale
provides
a measure
of nonverbal
cognitive
abilities;
little or no verbal
response
is required
by the child.
The Scale
consists
of seven
subtests
(Picture
Completion,
Coding,
Picture
Arrangement,
Block Design,
Object
Assembly,
Symbol
Search,
and Mazes),
all of which
assess
nonverbal
reasoning and problem-solving.
Other
specific skills assessed
include
visualspatial
perception
and organization
(eg, Picture
Completion,
Block
Design, Object
Assembly,
Mazes,
Symbol Search);
visual
sequencing
(eg,
Picture
Arrangement,
Coding);
visual-motor
coordination
(eg, Coding,
Block Design,
Object
Assembly,
Mazes);
attention,
concentration,
and
short-term
memory
(eg, Coding,
Picture Completion);
and psychomotor
speed of processing
nonverbal
information
(eg, Block Design,
Object
Assembly,
Coding,
Symbol
Search,
Mazes).
Different profile patterns suggest
different
types of cognitive
impairments.
For example,
mentally
retarded
children
generally
will have
depressed
scores
across
all subtests,
with no significant
discrepancy
between the Verbal
and Performance
domains.
Children
who have learning
disabilities
tend to have average
or
above average
FSIQs
and may have a
significant
difference
between
VIQ
and PIQ or significant scatter among
the subtests
within
either
scale. Most
commonly,
these children have lower
Verbal scores than Performance
scores
(consistent
with reading,
spell-
Pediatrics in Review
Vol. 16
No. 9
Downloaded from http://pedsinreview.aappublications.org/ at University of Connecticut on May 26, 2015
Septe,nber
1995
.
.
ACHIEVEMENT
ing, or arithmetic
disabilities),
although
the reverse
pattern
can occur among
children
who have
impaired
visual-perceptual
abilities
(ie, lower
Performance
than Verbal
scores).
The subtest
scores
on the WISC
III also can be grouped
by index
scores,
which
provide
more
information
about
the pattern
of cogni-
Vol. 16
No. 9
Two of the most common
achievement tests used are the Wide Range
Achievement
Test-3
(WRAT-3)
and
the Woodcock-Johnson
Psycho-Educational
Battery-Revised.’
16 The
WRAT-3
is a brief, easily administered test of reading,
spelling,
and
arithmetic
that was restandardized
in
1993 and has high test-retest
reliability and satisfactory
validity.
It provides standardized
scores
(mean
100, standard
deviation
=
15), percentile
ranks,
and grade equivalents.
Scores
falling
within
1 standard
deviation of the mean,
or between
the
16th and 84th percentile
rank, are
considered
to be within
the normal
range.
The percentile
rank achieved
indicates
the level at which
a child
performed
compared
with other children in the normative
group. Thus, if a
child scored
at the 55th percentile,
he
or she performed
as well as or better
than 55% of the normative
group,
but
not as well as 45% of the normative
group.
In terms of grade equivalents,
a grade equivalent
score within
1
year of actual
grade level is considered average,
while a grade equivalent 2 or more years below
actual
grade level is considered
delayed.
Because the WRAT-3
is a brief measure,
it is used best for academic
screening,
but should
not be used alone for planfling remediation.
The Woodcock-Johnson
is a comprehensive
assessment
measure
that
consists
of 27 subtests
in three categories:
Tests of Cognitive
Ability,
Tests of Achievement,
and Tests of
Interest
Level.
The battery
is designed
for those aged 2 years to adulthood. The Tests of Achievement
are
the most useful component
of the
.
tive problems.
These
scores
include
the Verbal
Comprehension
Index
(comprised
of Information,
Similarities,
Vocabulary,
and Comprehension scores),
the Perceptual
Organization
Index
(comprised
of Picture
Completion,
Picture
Arrangement,
Block
Design,
and
Object
Assembly scores),
the Freedom
From
Distractibility
Index
(comprised
of
Arithmetic
and Digit
Span scores),
and the Processing
Speed
Index
(comprised
of Coding
and Symbol
Search
scores).
Significant
discrepancies
among
index
scores
can highlight
strengths
and weaknesses
and clarify
learning
and attention
deficit
disorders
further.
For
example,
children
who have attention deficit
disorder
and hyperactivity
often
have lower
scores
on
the Freedom
From
Distractibility
Index
than on the other
indices.
Intelligence
tests alone,
however,
do not provide
enough
information
for diagnosis
or the planning
of
treatment. There is no one type of
WISC
III profile that applies to all
cases
of learning disabilities. The
discrepancy
between ability and
achievement
probably is the best
indicator of learning disability.
Therefore,
measures of both intellectual
functioning
and academic
achievement are needed
to determine
whether
the child’s
intellectual potential
is consistent
with his or her
school performance. For example, a
child who has average
or above
average intellectual
abilities
but scores
below
average
on tests of achievement is not able to learn information
and perform
at the level of his intellectual
potential.
His scores
on the
achievement
and intelligence tests
can be compared
to determine if this
is due to a specific learning disability (eg, in reading, spelling, or math)
or to a more pervasive
problem
of
selective attention and concentration.
Pediatrics in Review
TESTS
The
Woodcock-Johnson
categories:
designed
for
test
the WRAT-R,
the results
are more
useful
for planning
academic
remediation.
Standard
scores
(mean
=
100, standard
deviation
=
15), percentile
ranks,
and grade norms
are
provided
for reading,
mathematics,
written
language,
knowledge,
and
skills.
As with other measures,
scores
within
1 standard
deviation
of the
mean are considered
to be within
the
range of normal,
as are scores
falling
between
the 16th and 84th percentile
ranks.
BEHAVIOR
SCALES
In addition
to measures
of intelligence
and achievement,
behavior
rating scales
are important
in an assessment battery.
These
scales
can
indicate
the child’s
behavioral
functioning
in the home and school
and
help interpret
the intellectual
and
achievement
measures.
Children
whose
intelligence
is average
or
above
and whose
school
performance
is poor may have an attention
deficit
or an emotional
problem
that is interfering
with school
performance.
Behavior
rating scales
can help identify
these difficulties.
The two scales
used most commonly
are the Child Behavior
Checklist (CBCL)
and the Connors
Rating
Scale.’7’
18 The
CBCL
includes
parent and teacher
forms for children
ages 4 to 16 years,
a parent
form for
children
ages 2 to 3 years,
a youth
self-report
form for those ages I I to
18 years,
and a direct
observation
form. Items are scored 2, 1, or 0
according to whether they are very
true, sometimes
true, or not true, and
they are plotted on a profile that consists of an Internalizing Scale and
is a measure
with
cognition,
achievement,
and interest.
those ages 2 years to adulthood.
battery
for assessing
school
achievement and learning
difficulties
because
their reliability
and validity
are satisfactory.
The Tests of Cognitive
Ability are reported
to have inadequate
construct
validity
and should
not be
substituted for other standardized
measures of intelligence. The
achievement
tests require 30 to 40
minutes to administer, and although
they take longer to administer than
September
CHILDDE1EL.OPMENT
Testing
three
It is
an Externalizing Scale, based on factor analysis.
The raw scores
can be
converted to T-scores, based on age
and gender. T-scores are standardized
scores that have a mean of 50 and a
standard deviation of 10. T-scores
above 70 are considered clinically
significant. Reliability and validity
data are satisfactory, although ratings
are based on parent, teacher, or selfperceptions.
1995
Downloaded from http://pedsinreview.aappublications.org/ at University of Connecticut on May 26, 2015
343
CHILD
DEVELOPMENT
Developmental
Testing
The Connors
Parent
Rating
Scale
was designed
for rating
the behavior of children
3 to 17 years of age.
It is available
in either
a long (93
items)
or short form (48 items).
In
addition,
an abbreviated
10-item
version,
referred
to as the Hyperactivity
Index,
is available
for screening and follow-up.
A teacher
rating
form,
the Connors
Teacher
Rating
Scale,
also is available
in long (39
items),
short (28 items),
and abbreviated
(10 items)
versions
for children 4 to 12 years.
Items
on both
the parent
and teacher
versions
are
rated 0, 1 2, or 3 if they occur
not
at all, just a little.
pretty
much,
or
very much.
Items
are grouped
into
factors
(eg, conduct
problem,
learning problem.
psychosomatic
problem, hyperactivity,
anxiety).
Raw
scores
can be converted
into
T-scores,
with a mean of 50 and a
standard
deviation
of 10. Age by
gender
normative
data are available,
with T-scores
above
70 considered
indicative
of behavior
problems
in
each factor
domain.
Reliability
and
validity
data are satisfactory
for the
factors
measured,
although
the hyperactivity
scale is the component
of this scale
used most commonly.
Rating
scales
can be particularly
useful
in the assessment
of attention
deficit
hyperactivity
disorder
because
they can reflect
behavior
in
multiple
settings
(eg, home,
school,
after-school
care),
as well as provide observations
by multiple
sources
(eg, parent,
teacher,
child
care provider).
In addition,
they
provide
a useful
way to monitor
a
child’s
response
to treatment.
For
example,
rating
scales
that are completed
before,
during,
and after
treatment
can document
changes
in
behavior
as a function
of the treatment provided.
The major
limitation
of behavior
rating
scales
is that
they are based
on perceptions
of the
rater and so are not totally
objective. If the rater (ie, the parent
or
teacher)
is not considered
to be reliable,
the results
cannot
be assumed
to be accurate.
This limitation can be controlled
by obtaining
multiple
ratings
by different
raters
in different
settings.
Thus,
for example,
if ratings
by a teacher
and a
child care provider
indicate
no hyperactivity,
but ratings
by a parent
,
344
endorse
hyperactivity,
the behavior
may be considered
situation-specific
(ie, at home
with parent)
rather
than an enduring
characteristic
of
the child.
This,
in turn, will influence the type of treatment
recommended.
FOLLOW-UP
specific
areas of developmental
functioning.
Throughout
this process, the pediatrician’s
role as advocate
for the child
and family
serves
as a bridge
to other professionals
and services,
with the ultimate goal of facilitating
the optimal
development
of the child.
ASSESSMENTS
Once
a comprehensive
assessment
battery
is completed,
a diagnosis
is
formulated,
and a treatment
plan is
designed,
follow-up
evaluations
should
be planned.
Children
who
have developmental
disabilities,
learning
disabilities,
or behavioral
problems
should
be assessed
repeatedly to determine
the progress
they
have made as a result
of intervention or as a function
of developmental
maturation.
Results
from
systematic
evaluations
can be used
to update
or revise
treatment
and to
determine
the needs
for the child’s
future
(eg, special
education,
social
skills
training,
vocational
training).
Summary
Pediatricians
play a central
role in
monitoring
the development
of infants and children
during
the course
of providing
well child care. Parents
turn to pediatricians
for help in determining
whether
their child has a temporary
lag in development,
a serious
delay or disorder,
or a significant
behavior
problem
that should
be addressed.
With the passage
of PL 99457, pediatricians
also play a key
role in referring
children
at risk to
early intervention
services.
By employing
a strategy
of developmental
surveillance,
with periodic
developmental
screening,
the pediatrician
can
determine
when a child should
be
referred
for more extensive
developmental
or psychological
testing,
which
will aid in the process
of diagnosis and treatment
of developmental
disabilities
and behavioral
disturbances.
Knowledge
of the screening
and testing
measures
used commonly,
as well as their limitations,
will result
in more accurate
interpretation
of the
data derived
from such measures.
Once delays
are diagnosed
and treatment is initiated,
repeated
assessments over time will serve to identify
areas in need of continuing
intervention while
indicating
gains
made
in
REFERENCES
I . Dworkin
P. British
and American
recommendations
for developmental
monitoring:
the role of surveillance.
Pediatrics. I989:84:1000-1010
2. Frankenburg
W, Dodds
J. The Denver
II:
a major
revision
and restandardization
of
the Denver
Developmental
Screening
Test.
Pediatrics. I992;89:9 1-97
3. Ireton
H, Thwing
E. The Minnesota
Child
Development
Inventory.
Minneapolis.
Minn:
Behavioral
Science
Systems;
1974
4. Newborg
J, Stock J, Wnek
L. Battelle
Developmental
Inventory.
Allen,
Tex:
DLM Teaching
Resources;
1984
5. Capute
AJ. Palmer
FB, Shapiro
BK, et al.
The Clinical
Linguistic
and Auditory
Milestone
Scale:
prediction
of cognition
in
infancy. Dev Med Child Neurol.
1986;28:
762
6. Coplan
J. ELM Scale:
The Early
Language
Milestone
Scale.
Tulsa,
OK: Education
Corporation;
1983
7. Frankenburg
W, Coons
C. Home
screening
questionnaire:
its validity
in assessing
home environment.
J Pediatr.
1986:108:
624-626
8. Jellinek
M, Murphy
J. Robinson
J. et al.
Pediatric
symptom
checklist:
screening
school-age
children
for psychosocial
dysfunction. J Pediatr. l988;l 12:201-209
9. Bayley
N. Manualfor
the Bavlev
Scales
of
Infant
Development.
Berkeley.
Calif:
Psychological
Corporation:
1969
10. Bayley
N. Bavlev
Scales
of Infant
Developmeat. Second
Edition.
San Antonio,
Tex:
The Psychological
Corporation;
1993
I 1. Knobloch
H, Stevens
F. Malone
A.
Manual
of Developmental
Diagnosis.
New
York,
NY: Harper
& Row;
1980
12. Wechsler
D. Manualfor
the Wechsler
Preschool
and Prima,’’
Scale of
Intelligence-Revised.
San Antonio,
Tex:
The Psychological
Corporation;
1989
13. Wechsler
D. Manual
for the Wechsler
Intelligence
Scale for Children
111. San
Antonio,
Tex: The Psychological
Corporation;
1991
14. Wechsler
D. Manual
for the Wechsler
Adult
Intelligence
Scale-Revised.
San
Antonio,
Tex: The Psychological
Corporation:
1981
15. Wilkinson G. Wide Range
Achievement
Test-3
Administration
Manual.
Wilmington.
Del: Jastak
Associates,
mc;
1993
16. Woodcock
RW, Johnson
MB. WoodcockJohnson Psycho-Educational
BatteryRevised.
Allen.
Tex: DLM Teaching
Resources;
1989
17. Achenbach
T. Manual
for the Child
Behavior
Checklist. Burlington,
Vt:
University
of Vermont;
1991
Pediatrics in Review
Vol.
16
No.
Downloaded from http://pedsinreview.aappublications.org/ at University of Connecticut on May 26, 2015
9
September
1995
CHILD
DEVELOPMENT
Developmental
I 8. Connors
K. Connors
York,
NY: Multi-Health
Rating
Scales.
New
Systems.
Inc;
Testing
PIR QUIZ
1989
9.
SUGGESTED
READING
Committee
on Children
With Disabilities.
Screening
for developmental
disabilities.
Pediatrics. l986;78:526-528
Frankenburg
W, Fandal
A, Thornton
S.
Revision
of Denver
prescreening
developmental
questionnaire.
J Pediatr. l987;1
10:
653-657
Gibbs
E, Teti D. interdisciplinary
Assessment
of Infants.
Baltimore,
Md: Paul H. Brookes
Publishing
Co; 1990
Glascoe
FP. Byrne
KE, Ashford
LG. et al.
Accuracy
of the Denver
II in developmental
screening.
Pediatrics. l992;89:
1221-1225
Meisels
S. Can developmental
screening
tests
identify
children
who are developmentally
at
risk? Pediatrics.
l989;83:578-585
Sattler
J. Assessment
of C’hildren
‘s Abilities.
San Diego,
Calif:
Jerome
M. Sattler,
Publisher;
1988
Strangler
SR. Huber
CJ, Roth DK. Screening
Growth and Development
of Preschool
Children: A Guide for Test Selection. New
York.
NY: McGraw-Hill;
1980
10.
When a test report
indicates
that a
child has an intelligence
quotient
or
developmental
quotient
between
85
and 1 15 and that the child, therefore, is ‘ ‘average,’
‘ it will
be appropriate
to conclude
that the child:
A. Does not need further testing.
B. Has scored
within
1 standard
deviation
of the average
(mean)
score for a reference
group.
C. Is neither
dull nor bright.
D. Is normal.
Among
the following
screening
tests, the one that appears
to be
best for the evaluation
of school
readiness
is the:
A. Battelle
Developmental
Inventory Screening
Test.
B. Denver
Developmental
Screening Test (DDST
II).
C. Early Screening
Inventory
(ES!).
D. Minnesota
Child Developmental
Inventory
(MCDI).
I 1 . When a developmental
test standardized
on a group of children
drawn
from an affluent
community
is applied
to children
from a lower
middle
class or economically
disadvantages
group.
the test likely
will
suffer most importantly
from
impaired:
A. Reliability.
B. Sensitivity.
C. Specificity.
D. Validity.
12.
A test that gives widely
divergent
results
on early repetition
with a
child who appears
to be in the
same
clinical
sions
may
A.
Reliability.
B.
Sensitivity.
C.
D.
Specificity.
Validity.
I 3. The
test
state
have
ability
with
can identify
in a clinical
on both
occa-
low:
which
a screening
all affected
persons
sample
is a measure
of
the test’s:
A. Reliability.
14.
B.
Sensitivity.
C.
D.
Specificity.
Validity.
The
ability
identify
clinical
IS.
of a screening
test
to
all nonaffected
persons
in a
sample
is a measure
of its:
A.
B.
Reliability.
Sensitivity.
C.
Specificity.
D.
Validity.
The ability of a test to measure
what it purports
to measure
is an
aspect
of its:
A.
B.
Reliability.
Sensitivity.
C.
Specificity.
D.
Validity.
IN BRIEF
Tongue-tie:
The
Tongue.
Human
Anomalies.
Management
Gorlin
Malformations
Volume
Ri,
Sedano
HO.
of a Short
In:
amid Related
II. Stevenson
RE,
Hall
JG, Goodman
RM, eds. New York, NY:
Oxford
University
Press;
1993:401-403
Tongue-Tie.
Catlin
Fl, De Haan V. Arch
Otolarvngol.
Assessment
I 97 1 :94:548
-557
of Lingual
Function
When
Ankyloglossia
(Tongue-tie)
Is Suspected.
Williams
WN, Waldron
MM. JADA.
1985;
I 10:353-356
Sublingual
Dimensions
in lnfants
and
Young
Children.
Fletcher
SG. Daly DA.
Arch
Otolarvngol.
I 974;99:292-296
Neonatal
Frenotomy
May Be Necessary
to
Correct
Breast
Feeding
Problems.
Marmet
C, Shell E, Marmet
R. J Human
Lact.
1990;
6:117-120
Tongue-tie,
or ankyloglossia,
historically has been believed
to cause
speech
defects,
as well as breastfeeding difficulties
and dental
problems.
St. Mark wrote, “The
string of his
tongue was loosed and he spoke
Pediatrics
in Review
Vol.
16
No.
9
September
Sublingual
Frenulum
plain,”
and midwives
in the 15th
century
reportedly
kept a fingernail
sharp to cut the frenula
of all newborns
in an attempt
to prevent
possible speech
problems.
Only within
the
last century
has it become
acceptable
not to perform
frenulotomy
for children who have ankyloglossia.
During
early development
the
tongue
is fused to the floor of the
mouth.
Cell death and resorption
free
the tongue,
with the frenulum
left as
the only remnant
of the initial attachment. Tongue-tie
results
from a short
and thickened
lingual
frenulum,
which
restricts
(or ties) movements
of the tongue.
Limitation
of movement may vary from very mild to
complete
fusion
of the tongue
to
the floor of the mouth. Fusion is referred
to as complete
ankyloglossia.
Tongue-tie,
really partial
ankyloglossia,
is defined
as a limitation
of
movement
severe
enough
that notching of the tip of the tongue
occurs
when an attempt
is made to protrude
it from the mouth.
The incidence
of significant
tongue-tie
has been estimated
to be
less than 0.5 per 1000. This still
should
be frequent
enough
for cornplications
to have been reported
in
the literature,
but no definitive
picture
has emerged
of partial
ankyloglossia
as a cause of speech
defects,
breastfeeding
difficulties,
or dental
problems. In fact, reviews
of the literature
generally
suggest
that ankyloglossia
is not the significant
cause of speech
defects
it was believed
to be historically.
Most speech
pathologists
feel
that partial
ankyloglossia
rarely inter-
1995
Downloaded from http://pedsinreview.aappublications.org/ at University of Connecticut on May 26, 2015
345
Developmental Testing
Kathleen E. Gilbride
Pediatrics in Review 1995;16;338
DOI: 10.1542/pir.16-9-338
Updated Information &
Services
including high resolution figures, can be found at:
http://pedsinreview.aappublications.org/content/16/9/338
Permissions & Licensing
Information about reproducing this article in parts (figures, tables) or in its
entirety can be found online at:
http://pedsinreview.aappublications.org/site/misc/Permissions.xhtml
Reprints
Information about ordering reprints can be found online:
http://pedsinreview.aappublications.org/site/misc/reprints.xhtml
Downloaded from http://pedsinreview.aappublications.org/ at University of Connecticut on May 26, 2015
Developmental Testing
Kathleen E. Gilbride
Pediatrics in Review 1995;16;338
DOI: 10.1542/pir.16-9-338
The online version of this article, along with updated information and services, is located on
the World Wide Web at:
http://pedsinreview.aappublications.org/content/16/9/338
Pediatrics in Review is the official journal of the American Academy of Pediatrics. A monthly
publication, it has been published continuously since 1979. Pediatrics in Review is owned, published, and
trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove
Village, Illinois, 60007. Copyright © 1995 by the American Academy of Pediatrics. All rights reserved.
Print ISSN: 0191-9601.
Downloaded from http://pedsinreview.aappublications.org/ at University of Connecticut on May 26, 2015