TUTOR GUIDE BASIC MEDICAL SCIENCE 1 (BMS1
advertisement

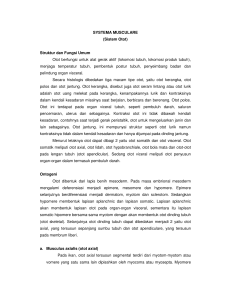
TUTOR GUIDE BASIC MEDICAL SCIENCE 1 (BMS1) KASUS 1 TIM BLOK BMS 1 Dr.drg.Sri Tjahajawati,MKes., Dr.drg.Marry S.Mariam,MS , Dr. Winny Yohana,drg.,SPKGA, Drg.Nani Murniati,MKes., drg.Moch.Rodian,MKes., drg.Tadeus Arufan Yasrin,MM., drg.Rosiliwati Wihardja MDSc., drg.Ervin Rizali.,MKes., drg.Kartika Indah Sari,MKes., Fakultas Kedokteran Gigi Universitas Padjadjaran Bandung- 2016 Kasus BMS 1 Kasus 1: Rani seorang remaja berumur 18 tahun datang bersama ibunya ke RSGMP FKG Unpad. Tadi pagi pasien jatuh dari sepeda motornya. Keluhan yang diutarakan adalah satu gigi rahang bawah sebelah kiri lepas serta gusi dan bibir berdarah akibat terbentur pada permukaan jalan. Dokter gigi yang bertugas ingin memeriksa rongga mulut pasien, tetapi pasien mengeluhsakit. Dokter gigi menemukan adanya luka terbuka di daerah rahang bawahkiripasien. Pertanyaan: 1. Masalah apa yang dialami remaja ini? 2. Buat hypotesanya. 3. Buatlah learning issues dari kasus ini Kasus 1 Tutor Guide TulangdanOtot Identitas pasien Pasien remaja perempuan, bernama Rani, usia 18 th. Masalah pasien: trauma pada jaringan lunak dan keras pada daerah mandibula. Pemeriksaan klinis: Ekstra oral: luka terbuka di daerah rahang bawah kiri Intra oral :satu gigi rahang bawah kiri lepas, gusi dan bibir berdarah Hipotesis: Gigi rahang bawah kiri lepas serta luka pada jaringan lunak karena trauma mekanis Mekanisme: Pasien terjatuh mengalami trauma mekanis menyebabkan satu gigi rahang bawah kiri lepas dan luka terbuka pada jaringan lunak. Trauma Jaringan Keras Jaringan Lunak Gigi Lepas Luka Terbuka Learning issues: Anatomi: 1. 2. 3. 4. Arahkan mahasiswa pada anatomi tulang cranium Menyebutkan anatomi rahang bawah Menyebutkan anatomi otot wajah Vaskularisasi dan persarafan rahang bawah Kuliah: menjelaskan cervicalis vertebrae dan fascia daerah leher (drg.Nani Murniati, MKes) Histologi: 1. Arahkan mahasiswa dengan pertanyaan yang menjelaskan secara mikroskopis jaringan tulang dan kartilago meliputi jenis pembentukannya (histogenesis) 2. Arahkan mahasiswa pada struktur mikroskopis dan jenis jaringan otot. 3. Arahkan mahasiswa untuk menjelaskan penyembuhan jaringan lunak dan tulang secara histologi Kuliah: menjelaskan sistem kontraksi jaringan otot Fisiologi: 1. Arahkan organisasi sistem kerangka dan otot dan 2. Menjelaskan mekanisme kerja kerangka otot 3. Menjelaskan fungsi kerangka dan otot Kuliah: Menjelaskan karakteristik kontraksi otot polos, otot lurik dan otot jantung Menjelaskan kelainan fungsi sistem kerangka dan otot Praktikum : 1. Anatomi : cranium, vertebra servikalis, otot-otot leher dan wajah (Tim) 2. Histologi: tulang, kartilago, dan otot (Tim) 3. Fisiologi: Refleks (Tim) ANATOMI TULANG DAN OTOT Rangka manusia terbagi dalam 3 golongan besar yaitu : 1. Cranium 2. Sceletum trunci / Batang badan 3. Sceletum ekstrimitas Cranium terbagi 2 kelompok 1. Neuro cranium Yaitu tulang-tulang yang melindungi otak terdiri : 2. - Os frontalis - Os ethemoidalis - Os occipitalis - Os sphenoidalis - Os temporalis - Os parietalis Splanchno cranium Yaitu tulang-tulang yang membentuk wajah, terdiri dari : - Os maxilla - Os mandibula - Os Nasalis - Os zygomaticus - Os lacrimalis - Concha nasalis inferior - Os vomer Os palatum merupakan tulang yang tidak termasuk kedalam kedua kelompok karena terletak antara neuro cranium dan splanchnocranium. 1. Gambar cranium 2. Gambar maxilla dan mandibula Otot-otot daerah wajah I. Kelompok Ortbital 1. M.Orbicularis occuli o Pars palpebral o Pars Orbitalis 2. M. Crorrugator supercilli II. Kelompok Nasalis 1. M. Nasalis o Pars transversa o Pars alar 2. M. Procerus 3. M. Depressor septi III. Kelompok Rongga Mulut 1. M. Depresor angguli oris 2. M. Depresor labii inferior 3. M. Mentalis 4. M.Risorius 5. M. zygomaticus mayor 6. M. zygomaticus minor 7. M. Levator labii superior 8. M. Lavetor labii superior alaquenasi 9. M. Lavetor anguli oris 10. M. Orbicularis oris 11. M. Buccinator IV. Kelompok Lain 1. M. Auricularis anterior 2. M. Auricularis superior 3. M. Auricularis posterior 4. M. Occipito frontalis - Frontal belly - Occipital belly Gambar Otot Wajah Leher Merupakan sebuah tabung yang berkesinambungan dari kepala sampai badan pada bagian dalam leher terdpat vertebra cervicalis otot pembuluh darah, saraf dan kelenjar endokren. Gambar : Vertabra Cervicalis terdiri dari 7 buah, C1 – C7. Batas-batas Leher Cranial : - Mentum - Margo inferior mandibulea - Angulus mandibulea - Proc Mastoidus - Linea nuchae superior Caudal : - Incisura yugularis sterni - Clavicula sinistra dan dextra - Articulatio clavico acromialis - Garis yang menghubungkan articulation claviculo acromialis dengan proc. spinosus vert. cervialis VII Pembagian Regioner Leher A. Regio anterior colli Os hyoid membagi otot-otot leher menjadi : 1. Otot-otot suprahyoid yaitu : - M. Stylohyoid - M. Digastricus venter anterior - M. Digastricus venter posterior - M. Mylohyoid - M. Geniohyoid 2. Otot-otot infrahyoid - M. Omohyoid - M. Sternohyoid - M. Thyrohyoid - M. Sternothyroid B. Regio anterior colli Daerah ini tertutup oleh : - M. Trapezius - M. Splenus capitis - M. Splenus cervicis - M. Levator scapulae Lapisan Fasia dileher : Superfisial fasia, adalah lapisan tipis yang mengelilingi otot platisma. Saraf cutaneous, pembuluh dan limp node terletak dalam fasia ini. Deep fasia, terletak dibawah superfisial fasia, yang akan membentuk investing layer di deep fasia, pretracheal fasia, prevertebral fasia dan carotid sheath. Histologi Bone Bone is one the hardest tissues of the human body, second only to cartilage in its ability to with stand stress Functions : 1. Support fleshly structures 2. Protect such vital organs 3. Harbors the bone marrow 4. Reservoir of calcium phosphat and others ions Composed : I. Bone Matrix II. Cells : • Osteocytes • Osteoblasts • Osteoclasts Bone Matriks 1. INORGANIC MATTER • Calcium Phosphat • Bicarbonaat • Citrate • Magnesium • Pottasium • Sodium 2. ORGANIC MATTER • Collagen Fibers • Amorphous Ground substance : a. Chondroitin 4-sulfate b. Chondroitin 6-sulfate c. Keratan Sulfate BONE CELLS 1. OSTEOBLASTS • Synthesis of bone matrix a. Type I Collagen b. Proteoglycans c. Glycoprotein • Located at the surfaces of bone tissue, side by side, in away that resembles simple epithelium • When actively : Cuboidal to columnar shape • When actively declines : Flatten OSTEOCYTES • Lie in the lacunae • One osteocytes in each lacuna • Canaliculi house cytoplasmic process • Processes of adjucent cell make contact via gap junction This figure is section of bone tissue showing an osteocyte with its cytoplasmic processes surrounded by matrix. Ultrastructure compatible with a low level of synthetic activity is apparent in both nucleus and cytoplasm. 3. OSTEOCLASTS • Very large • 5 to 50 contain nuclei • Lie in howship’s lacunae • Derived from the fusion of monocytes • Secrete : a. Acid b. Collagenase c. Other proteolytic enzymes PERIOSTEUM AND ENDOSTEUM External and intrnal surfaces of bone are covered by layers of bone forming cells and connective tissue called periosteum and endosteum. 1. Periosteum Outer Layer - Collagen fibers Bundle : Sharpey’s fibers - Fibroblasts Inner Layer More celllular (oteoprocenitor cells) is composed of flattened cells to divided into osteoblasts 2. cells (single layer) a. Small amount of connective tissue Therefore, the endosteum is consider ably thinner than the 3. periosteumEndosteum Lines all internal surfaces of cavities with in the bone Composed : Osteoprogenitor Functions of periosteum and endosteum : 1. Nutrition of osseus tissue 2. Supply of new osteoblasts for repair or growth of bone Schematic drawing of the wall of a long bone diaphsis. Type of bone A. MICROSCOPIC EXAMINATION 1. Primary, immature or woven bone 2. Secondary, mature or lamellar bone B. GROSS OBSERVATION (CROSS SECTION) 1. Dense area without cavities : Compact Bone 2. Areas with numerous interconecting cavities : Cancellous (spongy) bone In long Bones : 1. Bulbous ends : Epiphyses Spongy bone covered by a thin layer of compact bone 1. Cylindrical Part : Diaphysis Almost totally composed of compact bone, with a small component of spongy bone on its inner surface around the bone marrow cavity. In Short Bones : Usually have a core of spongy bone completely surrounded by compact bone. In Flat Bones (Calvaria) Have two layers of compact bone called plated (tables), separated called the diploe. PRIMARY BONE TISSUE First bone tissue Temporary, replace by secondary bone tissue, except : - Near the sutures of the flat bones of the skull - In tooth sockets - In the insertion some tendons Characteristics : - Irregular array of collagen fibers - Smaller mineral content - Higher proportion of osteocytes than in secondary bone tissue SECONDARY BONE TISSUE - Collagen fibers : Lamellae - Haversian canals - Haversian system or osteon - Lacunae The lamellae exhibit a typical organization consisting of : 1. Haversian system 2. Outer circumferential lamellae 3. Inner circumferential lamellae 4. Intertitial lamellae The haversian canal communicate with : 1. The narrow cavity 2. The periosteum 3. The volkman’s canals (do not have concentric lamellae) Schematic drawing of the wall of a long bone diaphsis. HISTOGENESIS Bone can be formaed in two ways : I. Direct mineralization of matrix secreted by osteoblasts (intra membranous ossification) II. Deposition of bone matrix preexiting cartilage matrix (endochondral ossification) I. Intramembranous Ossification formed by intramembranous ossification : • The frontal and parietal bones of the skull • The occipital and temporal bones of the skull • The mandible and maxilla The Beginning of Intramembranous Ossification II. Endochondral Ossification Takes place within a piece of Hyalin Cartilage whose shape resembles a small version or model of the bone to be formed. Endochondral ossification consists of two phases : 1. The first phase Hypertrophy and destruction of the chondrocytes of the model of the bone, leaving expanded lacunae separated by septa of calcified cartilage matrix. 2. The second phase THE OSSIFICATION CENTRE 1. Primary ossification centre appears in the diaphysis 2. Secondary ossification centre arises at the centre of each epiphysis When the bone tissue that originated at the secondary centres occupies the epiphysis, cartilage remains restricted to 2 places: 1. Articular cartilage - Persist throughout adult life - Does not contribute to bone formation 2. Epiphyseal cartilage or the epiphyseal plate - Connect epiphysis to diaphysis - As the cartilage grows, it is replace continously by newly formed bone matrix mainly from the diaphyseal centre Schematic drawings showing the 3-dimensional shape of bone spicules in the epiphyseal plate area. Hyaline cartilages is stipple, calcifed cartilage is black, and bone tissue is shown in color. The upper drawing shown the region represented 3-dimensionally in the lower drawing. Epiphyseal cartilage, divided into five zones : 1. Resting zone • With out morphologic changes in the cells 2. Proliferative zone • Chondrocytes devided rapidly • Form columns of stacked cells parallel to the long axis of the bone 3. Hypertrophic cartilage zone • Large chondrocytes who cytoplasm has accumulated glycogen • The resorbed matrix is reduced to thin septa 4. Calcified cartilage zone • Simultaneous with the death of chondrocytes • The thin septa become calcified 5. Ossification zone • Endochondral bone tissue appears • Blood capillaries and osteoprogenitor cells formed by mitosis of cells originating from the periosteum invade the cavities • The osteoprogenitor cells form osteoblasts • Osteoblasts turn form a discontinuous layer over the septa • Over these septa, the osteoblasts deposit matrix MECHANISMS OF CLASSIFICATION Bone calcium is mobilized by two mechanisms : 1. Rapid Mechanism The simple transference of ions from hydroxyapatite crystal to interstitial fluid into the blood 2. Slow Mechanism Depends on the action hormones a. Parathyroid hormone Activates and increases the number of cells (osteoclasts) promoting resorption of the bone matrix with the consequent liberation of calcium b. Calcitonin Inhibits matrix resorption (its effect, is the opposite of parathyroid hormone) FRACTURE REPAIR When fractures : • The damaged blood vessels product a blood clot • Destruction of bone cells • Death of Bone cells During repair : • The blood clot, cells and damaged bone matrix are removed by macrophages Repair of a fractured bone by formation of new bone tissue through periosteal and endosteal cell proliferation MUSCLE TISSUE Muscle tissue is composed of differentiated cell containingcontractile proteins. The structural biology of these proteinsgenerates the forces necessary for cellular contraction, which drives movement within certain organs and the body as a whole muscle kinds - Smooth muscle - Skeletal muscle - Cardiac muscle Smooth muscle ; consists of collection of fusiform cells that in the light microscope, do not show striatims Their contraction process is slow and not show subyect to voluntary control. The cytoplasm of muscle cells (exluding the Myofibri) is called sarcoplasm, and the smooth endoplasmic reticulum is called sarcoplasmic reticulum. The sarcolemma is the cell membrane or plasmalemma Skeletal muscle : is composed of bundles of very long,Cylindrical, multinucleated cells that show cross-striations. Their contraction is quick, forceful, and usually under voluntary, control. It is caused by the interacrions of this actin filaments and thick myosin filaments whose molecular configuration allow them to slide upon one another. The forces necessary for sliding are generated by weak interactions in the bridges that bind actin to myosin. Cardiac muscle : also has cross-striations, and is composed of elongated, branched individual cells that lie parallel to each other. At sites of end to end contract are the intercalated disks, structures found only in cardiac muscle. Cardiac muscle contraction is involuntary vigorous, and rhythmic INNERVASI 1. MULTI - UNIT 2. TYPE – VISCERAL SKELETAL MUSCLE Macroscopic - Muscle fibre of red - Muscle fibre of white - Muscle fibre of transition Shape :to lie diagonal Drawing of to lie diagonal line multynuclear nucleus in the side Shape of to lie diagonal skeletal muscle sheaf Diagram of a segment of mammalian skeletal muscle. The sarcolemma and muscle fibrils are partially cut,showing the following components: The invagination of the T system (show in color: T and 5) occur at the level of transition between the A and I bands twice in every sacomere. They associate with terminal cisternae of the sarcoplasmic reticulum (3), formingtriads. Abundant mitochondria (4) lie between the myofibrils. The cut surface of the myofibrils (1) shows the thin and thick filaments. Surrounding the sarcolemma are a basal lamina (7) and reticular fibers (8). (Reproduced, with permission, from Krstic RV:Ultrastructure of the Mammalian Cell Springer-Verlag, 1979) Initiation of muscle contraction occurs by the binding of Ca2+ to the TnC unit of troponin, which exposes the myosin binding site on action (cross-hatched area). In a second step, the myosin head binds to action and the ATP breaks down ADP, yielding energy, which produces a movement of the myosin head. As a consequence of this change in myosin, the bound thin filaments slide over the thick filaments. This process, which repeats itself many times during a single contraction, leads to a complete overlapping of the action and myosin a resultant shortening of the whole myofiber Diagram of a section of heart muscle, showing central nuclei and intercalated disks HISTOGENESIS AND REGENERATION OF MUSCLE TISSUE Histogenesis • Smooth muscle : mesenchym tissue --->myoblast • Skeletal muscle : myoblast ---> sinsytium • Cardiac muscle : splanchnopleura (myoblast) Regeneration • Smooth muscle : - muscle cell - mesenchym cell • Skeletal muscle : - nucleus + sarcoplasma - in charge myoblast • Cardiac muscle : - very difficult 3.Fisiologi Sistem Rangka dan Otot 3.1 Pendahuluan Sistem rangka bersama-sama sistem otot membangun dan membentuk tubuh secara keseluruhan. Sistem kerangka dibungkus oleh sistem otot yang bertanggung jawab dalam fungsi gerakan tubuh melalui fungsi khusus, yaitu kontraksi otot. 3.2 Maksud dan Tujuan Mahasiswa harus mengetahui dan mempunyai kompetensi dalam : 1. Organisasi sistem kerangka dan otot. 2. Menjelaskan mekanisme kerja dan fungsi sistem kerangka dan otot. 3. Karakteristik kontraksi otot polos, otot lurik dan otot jantung. 4. Menjelaskan kelainan fungsi sistem kerangka dan otot. 3.3 Kegiatan 3.3.1 Sistem Kerangka Sistem kerangka dibangun oleh struktur tulang yang terdiri dari : tulang tengkorak, tulang belakang, tulang dada, tulang rusuk, tulang bahu, tulang belikat, tulang ekstremitas atas dan bawah, serta tulang panggul. 3.3.1.1 Fungsi Sistem kerangka Sistem kerangka berfungsi : 1. Sebagai penyokong struktur tubuh dan memberikan bentuk pada tubuh 2. Melindungi organ organ dalam yang lunak dan penting 3. Sebagai pengungkit yang pasif dalam pergerakan tubuh 4. Sebagai gudang penyimpan mineral seperti kalsium dan fosfor. 3.3.1.2 Fungsi sendi Sendi adalah jaringan penyambung yang berfungsi menghubungkan tulang dengan tulang, sebagai tempat pertemuan tulang dengan tulang yang befungsi untuk pergerakan sistem kerangka tubuh. Jenis pergerakan sendi yaitu : 1. Fleksi: gerak membengkok ke depan 2. Ekstensi: gerak meluruskan dari gerak fleksi 3. Abduksi: gerak ekstremitas menjauhi garis tengah tubuh. 4. Aduksi: gerak mendekat garis tengah tubuh 5. Rotasi: gerak memutar pada sumbu sentral. 3.3.1.3 Kelainan Tulang Kelainan yang terjadi pada tulang diakibatkan beberapa faktor, diantaranya : 1. Gangguan hormon pertumbuhan : dwarfism, gigantism 2. Gangguan hormon tiroid : kretinisme, goiter 3. Gangguan hormon paratiroid : gangguan. kalsifikasi 4. Gangguan metabolisme kalsium : rakhitis, osteomalasia, osteoporosia 5. Gangguan sikap kerja : deformitas tulang belakang 3.3.2 Sistem Otot Otot adalah jaringan yang melekat pada tulang yang mengisi hampir setengah dari berat badan. Otot adalah alat gerak aktif yang berfungsi menggerakkan tubuh dan organ dalam manusia. 3.3.2.1Fungsi Spesifik Sistem Otot Kemampuan bergerak adalah aktivitas esensial tubuh manusia yang dimungkinkan oleh fungsi unik dari otot yaitu fungsi kontraksi. Semua jenis otot pada umumnya memiliki tiga karakteristik : 1. Sifat kontrakbilitas : Bila otot berkontaksi maka jarak atau ruang antar jaringan berkurang. 2. Sifat ekstensibilitas : kemampuan otot untuk meregang. 3. Sifat elastisitas : kemampuan otot untuk kembali ke panjang semula bila otot berelaksasi. Ke-3 sifat otot tersebut menghasilkan gerakan tubuh. 3.3.2.2 Jenis Otot Pada prinsipnya semua gerakan tubuh ditentukan oleh tiga jenis otot, yaitu : otot rangka, otot polos, otot jantung. 1. Otot Rangka Otot rangka, adalah otot sadar melekat pada tulang rangka. Dibentuk oleh sejumlah serat yang diameternya berkisar dari 10 – 80 mikrometer. Bagian-bagian dari otot rangka meliputi: a. Sarkolema: membran sel dari serat otot yang terdiri dari membran plasma dan lapisan tipis bahan polisakarida yg mengandung serat kolagen tipis. b. Miofibril; filamen aktin dan miosin : Serat otot mengandung ratusan sampai ribuan miofibril yg terletak berdampingan dan memiliki filamen miosin dan aktin. Filamen tsb merupakan molekul protein polimer besar yg bertanggung jawab untuk kontraksi otot. Filamen-filamen tsb saling bertautan menyebabkan miofibril memiliki pita terang dan gelap. c. Sarkoplasma Sarkoplasma adalah miofibril-miofibril yang terpendam dalam serat otot di suatu matriks. Cairan sarkoplasma mengandung kalium, magnesium, fospat, dan enzim protein Gambar 1 Otot Rangka dan Gelendong Otot (potongan transversal). ( Sumber : Marieb, E.N; Hoehn, K. 2007. Human Anatomy & Physiology ) Gambar 2. Otot Rangka dan Motor Endplate ( Sumber : Marieb, E.N; Hoehn, K. 2007. Human Anatomy & Physiology ) 2. Otot polos, Otot polos adalah otot tak sadar ditemukan pada dinding organ dalam seperti lambung, usus, pembuluh darah. Jaringan otot polos mempunyai serabut-serabut (fibril) yang homogen sehingga bila diamati di bawah mikroskop tampak polos atau tidak bergaris-garis, ukuran berdiameter 2 sampai 5 mikrometer dan panjang hanya 20 sampai 500 mikrometer. Nukleusnya terdapat di tengah. Terdiri dari kumpulan sel fusimormis. Bila otot polos dirangsang, reaksinya lambat. Otot polos berkontraksi secara refleks dan dibawah pengaruh saraf otonom. Otot polos mendapat inervasi dari saraf simpatis dan parasimpatis. Otot polos terdapat pada saluran pencernaan, dinding pembuluh darah, saluran pernafasan. Fungsi otot polos biasanya mempunyai kegiatan spontan bila tidak ada perangsangan syaraf, karena itu suplai sarafnya berfungsi untuk mengubah kegiatan tersebut dan tidak untuk memulainya. Sel otot polos tesebar dalam jaringan penyambung tertentu, misalnya prostat. Gambar 3 Lapisan Otot Polos Usus Halus ( Sumber : Marieb, E.N; Hoehn, K. 2007. Human Anatomy & Physiology ) Pengaturan Saraf Terhadap Kontraksi Otot Polos Walaupun otot rangka diaktifkan secara eksklusif oleh sistem saraf, tetapi otot polos dapat dirangsang untuk berkontraksi oleh berbagai jenis sinyal: sinyal saraf, rangsangan hormonal, regangan otot, dan lain-lain. Penyebab utama ini adalah karena membran otot polos mengandung banyak jenis protein reseptor yang dapat menimbulkan proses kontraksi. Serat-serat saraf otonomik yang mempersarafi otot polos umumnya bercabang secara difus pada puncak lembaran serat otot. Substansi transmiter yang disekeresi oleh saraf otonom yang memepersarafi otot polos adalah asetikolin dan norepinefrin, tetapi keduanya tidak pernah disekresi oleh serat saraf yang sama. 3. Otot Jantung Otot jantung adalah otot tak sadar ditemukan hanya pada jantung. 3.3.3 Kelainan Otot Jenis kelainan yang terjadi pada otot rangka diantaranya : atrofi otot, hipertrofi otot, spasme otot, tetanus, distrofi otot, myasthenia gravis.