Uploaded by
common.user83500
Low Antithrombin Activity Predicts Hypertensive Disorders in Pregnancy
advertisement

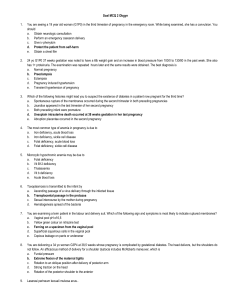
Received: 4 March 2019 | Revised: 12 July 2019 | Accepted: 23 September 2019 DOI: 10.1002/ijgo.12980 CLINICAL ARTICLE Obstetrics Low antithrombin activity before delivery predicts subsequent hypertensive disorders in pregnancy Mamoru Morikawa* | Takeshi Umazume | Kinuko Nakagawa | Kentaro Chiba | Satoshi Kawaguchi | Hidemichi Watari Department of Obstetrics and Gynecology, Hokkaido University Graduate School of Medicine, Sapporo, Japan *Correspondence Mamoru Morikawa, Department of Obstetrics and Gynecology, Hokkaido University Graduate School of Medicine, Sapporo, Japan. Email: [email protected] Abstract Objective: To examine whether laboratory parameters can predict the onset of recurrent hypertensive disorders of pregnancy (HDP). Methods: A retrospective study of 257 women with consecutive deliveries at a hospital in Sapporo, Japan, between 2009 and 2017. Women were divided into four groups according to whether or not they had HDP in the first and second peripartum periods (HDP-­HPD, HDP-­Non, Non-­HDP, Non-­Non). HDP was defined as gestational hypertension and/or proteinuria. Laboratory parameters measured on the day of or 1 day before delivery were compared between peripartum-­1 and peripartum-­2. Results: Frequency of HDP in peripartum-­2 was higher among the 24 (9.3%) women with HPD in peripartum-­1 (6/24, 25.0%) than among the 233 (90.7%) women without (3/233, 1.3%) (P<0.001). In peripartum-­1, women with HDP had lower median antithrombin activity than those without (74% vs 89%, P=0.021). Antithrombin activity in peripartum-­1 was also lower in the HDP-­HDP (67%) than in the HDP-­Non (79%) group (P=0.021). Antithrombin activities of 77% or less at the first delivery predicted HDP in peripartum-­1 (P<0.001) and 70% or less predicted HDP in peripartum-­2 (P=0.018). Conclusion: Women with HDP in peripartum-­1 had a higher incidence of HDP recurrence. Low antithrombin before a first delivery might predict recurrent HDP in a second pregnancy. KEYWORDS Antithrombin activity; Gestational hypertension; Hematocrit; Hypertension disorders of pregnancy; Platelet count; Predictor; Recurrence; Uric acid 1 | INTRODUCTION first peripartum period often fear recurrent HDP in a subsequent pregnancy, and past reports have revealed a high rate of recurrent The incidence of hypertensive disorders of pregnancy (HDP) is approx- HDP.3–11 Therefore, parameters for predicting the likelihood of recur- imately 5%–10% in high-­income countries.1 Globally, approximately rent HDP are needed. 50 000 women die from HDP or diseases associated with it (e.g., Women with HDP often have lower levels of fibrinogen or higher eclampsia, HELLP [hemolysis, elevated liver enzymes, low platelet levels of C reactive protein (CRP) at first delivery, and these markers count] syndrome, and acute fatty liver of pregnancy) each year.2 As a can be used to predict recurrent HDP.11 However, pregnant women result, women with severe HDP sometimes experience adverse out- may also have low fibrinogen owing to obstetric disseminated intra- comes, even in high-­resource countries. Women with HDP in their vascular coagulation after massive bleeding at delivery, or high CRP Int J Gynecol Obstet 2019; 1–7 wileyonlinelibrary.com/journal/ijgo © 2019 International Federation of Gynecology and Obstetrics | 1 2 | Morikawa ET AL. owing to infection in utero, among other reasons. Thus, new parame- Board of Hokkaido University Hospital (018-­0289). All women pro- ters to predict the onset of recurrent HDP are needed. vided informed consent for the use of their data in the study. Women with HDP often have high levels of hematocrit and uric Pregnant women with consecutive (first and second) deliveries were acid, low platelet counts, and/or low antithrombin activity.12 The divided into the four following groups according to whether or not they Guidelines for Obstetric Practice in Japan pose the following clinical experienced HDP in pregnancy: HDP-­HDP, HDP in peripartum-­1 and question “what cautions are required for the diagnosis and treatment peripartum-­2; HDP-­Non, HDP in peripartum-­1 only; Non-­HDP, HDP of pre-­eclampsia?”.13 The guidelines recommend that clinicians “repeat- in peripartum-­2 only; and Non-­Non, no HDP in either pregnancy. The edly assess physical findings (blood pressure and maternal weight), characteristics and parameters of these four groups were compared. blood tests (platelet, antithrombin activity, aspartate aminotransfer- HDP was defined as the presence of gestational hypertension ase, lactose dehydrogenase, and urate levels), and urine tests (protein/ and/or significant proteinuria. HDP was diagnosed in accordance creatinine ratio) for the mother and the development and wellbeing of with the classic criteria of the Japan Society of Obstetrics and the fetus (recommendation level B).13 The aim of the present study was Gynecology14 which was revised in May 1 2017 (but remained valid therefore to assess whether any of these laboratory parameters might until March 31 2018), and thereafter as the occurrence of systolic be promising candidates for predicting the likelihood of recurrent HDP. blood pressure of 140 mm Hg or higher and/or diastolic blood pressure 90 mm Hg or higher. Gestational hypertension was defined as hypertension occurring on the day of or after 20 gestational weeks; 2 | MATERIALS AND METHODS significant proteinuria was defined as either a spot-­urine protein/ creatinine ratio of more than 0.27 or more than 0.3 g of protein in In a retrospective observational study, data were assessed from 24 hours of urine collection. HDP was diagnosed for women who women who underwent consecutive deliveries on the day of or after developed hypertension with or without significant proteinuria on 22 gestational weeks at Hokkaido University Hospital, Sapporo, the day of or after 20 weeks and encompassed both gestational Japan, between January 1, 2009, and December 31, 2017. The study hypertension and pre-­eclampsia. Pre-­eclampsia was characterized was conducted after receiving approval from the Institutional Review by the presence of both hypertension and proteinuria. TABLE 1 Characteristics of the study women.a HDP in first pregnancy Characteristic All women (n=24)b HDP-­HDP (n=6)c No HDP in first pregnancy HDP-­Non (n=18)d All women (n=233)e Non-­HDP (n=3)f Non-­Non (n=230)g P value<0.05 1st delivery Primipara 20 (83.3) Maternal age, y 35 (23–39) Pre-­pregnancy BMI 21.2 (6.6–48.8) GA, wk 36 (24–41) Cesarean 20 (83.3) 5 (83.3) 35 (27–37) 23.7 (17.7–48.8) 32 (24–39) 6 (100) 15 (83.3) 35 (23–39) 184 (79.0) 30 (8–44) 2 (66.7) 35 (22–38) 21.1 (16.6–30.9) 20.6 (13.7–38.5) 23.1 (21.8–26.4) 37 (24–41) 14 (77.8) 38 (24–41) 120 (51.5) 37 (37–38) 3 (100) 182 (70.8) 30 (18–44) b vs e; d vs g 20.6 (13.7–38.5) 38 (24–41) 117 (50.9) b vs e; c vs g b vs e; c, d vs g 2nd delivery Maternal age, y Pre-­pregnancy BMI GA, wk Cesarean Interval 1st del. to 2nd pregn., mo 37 (25–40) 38 (30–40) 21.8 (17.0–50.3) 24.7 (18.5–50.3) 37 (26–39) 21 (87.5) 22.2 (2.8–41.9) 37 (29–38) 6 (100) 23.9 (14.9–38.4) 37 (25–40) 34 (20–46) 39 (25–42) 21.7 (17.0–35.0) 21.1 (14.5–39.7) 24.0 (23.3–24.3) 37 (26–39) 15 (83.3) 21.7 (2.8–41.9) 38 (31–41) 132 (56.7) 21.7 (2.1–85.7) 34 (31–37) 3 (100) 35.1 (25.6–44.7) 34 (20–46) b vs e 21.1 (14.5–39.7) 38 (31–41) 129 (56.1) b vs e; c, e vs g; d vs f b vs e; c, d vs g 21.4 (2.1–85.7) Abbreviations: BMI, body mass index (calculated as weight in kilograms divided by the square of height in meters), GA, gestational age; HDP, hypertensive disorders of pregnancy; Non, no hypertensive disorders of pregnancy. a Values are given as median (range) unless otherwise stated. b all women with HDP in peripartumn-1. c women with HDP in peripartumn-1 and peripartumn-2. d women with HDP in peripartumn-1 only. e all women without HDP in peripartumn-1. f women with HDP in peripartumn-2 only. g women without HDP in either pregnancy. | Morikawa ET AL. TABLE 2 3 Neonatal outcomes among the study women.a HDP in first pregnancy Outcome All women (n=24)b No HDP in first pregnancy HDP-­HDP (n=6)c HDP-­Non (n=18)d All women (n=233)e Non-­HDP (n=3)f Non-­Non (n=230)g P value<0.05 1st delivery Birthweight, g 2184 (354–4436) 1428 (618–4436) 2237 (354–3330) 2826 (420–4225) 2975 (2520–3010) 2823 (420–4225) b vs e; c, d vs g 5-­min Apgar score <8 0 (0.0) 0 (0.0) 2 (11.1) 21 (9.0) 0 (0.0) 21 (9.1) Stillbirth or END 2 (8.3) 0 (0.0) 2 (11.1) 13 (5.6) 0 (0.0) 13 (5.9) 2nd delivery Birthweight, g 2710 (843–3535) 2365 (1056–3535) 2810 (843–3305) 2915 (1362–4015) 1756 (1362–2595) 2922 (1680–4015) 5-­min Apgar score <8 0 (0.0) 0 (0.0) 0 (0.0) 6 (2.6) 0 (0.0) 6 (2.6) Stillbirth or END 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) f vs g Abbreviations: END, early neonatal death; HDP, hypertensive disorders of pregnancy; Non, no hypertensive disorders of pregnancy. a Values are given as median (range) or number (percentage) unless stated otherwise. b all women with HDP in peripartumn-1. c women with HDP in peripartumn-1 and peripartumn-2. d women with HDP in peripartumn-1 only. e all women without HDP in peripartumn-1. f women with HDP in peripartumn-2 only. g women without HDP in either pregnancy. Medical records were retrospectively reviewed for maternal and (HDP-­HDP group), 18 (7.0%) women had HDP only in peripartum-­1 obstetric characteristics (age, body mass index [BMI, calculated as (HDP-­Non group), 3 (1.2%) women had HDP only in peripartum-­2 weight in kilograms divided by the square of height in meters], parity, (Non-­HDP group), and 230 (89.5%) women did not experience mode of delivery) and blood test results (platelet counts, hematocrit, HDP (Non-­Non group). antithrombin activity, and uric acid). All parameters were measured The incidence of HDP in peripartum-­2 was significantly higher either 1 day before or on the day of delivery (hereafter “day −1/0”). among the 24 (9.3%) women with HDP in peripartum-­1 (HDP-­HDP and The recurrence rate of HDP, including gestational hypertension and HDP-­Non; 6/24, 25.0%) than among the 233 (90.7%) women without pre-­eclampsia, was evaluated for the four study groups. HDP in peripartum-­1 (Non-­HDP and Non-­NON; 3/233, 1.3%; P<0.001). JMP Pro 14 (SAS Institute, Cary, NC, USA) was used to perform statistical analyses. The data were presented as median (range) or number (percentage). Tukey–Kramer honestly significant difference (HSD) test or Mann-­Whitney U test was used to compare median values among the four groups. Fisher exact test was used to compare 3.2 | Characteristics of women with and without HDP in the first pregnancy As compared with women without HDP in peripartum-­1 (233/257, categoric variables. The Pearson product–moment correlation coeffi- 90.7%), those with HDP (24/257, 9.3%) were significantly older in cient was used to determine linear correlations between two variables. both the first (35 [23–39] years vs 30 [18–44] years, P=0.003) and Receiver operating characteristic (ROC) curves were used to assess second (37 [25–40] years vs 39 [25–42] years, P=0.002) pregnan- the ability of antithrombin activity at day −1/0 to predict the likelihood cies (Table 1). Gestational age was also significantly higher among of HDP in peripartum-­2. In all analyses, a P value of less than 0.05 was women with HDP than among those without HDP in peripartum-­1 taken to indicate statistical significance. for both the first (36 [24–41] years vs 38 [24–41] weeks, P=0.020), and second (37 [26–39] weeks vs 38 [31–41] weeks, P=0.007) 3 | RESULTS 3.1 | Recurrent HDP Among 2655 pregnant women who delivered during the study ­pregnancies (Table 2). In contrast, there were no significant differences in pre-­pregnancy BMI for either the first or second pregnancy, or in the time between the first delivery and second pregnancy (22.2 [2.8–41.9] months vs 21.7 [2.1–85.7] months, P=0.483) between women with and those period, 257 (9.7%) had consecutive deliveries. Among these, 6 without HDP in peripartum-­1 (Table 1). Birthweight was lower for (2.3%) women had HDP in both peripartum-­1 and peripartum-­2 women with HDP in peripartum-­1 than for women without HDP in 4 | Morikawa ET AL. (A) specificity, positive predictive value (PPV), and negative predictive value (NPV) were 0.625, 0.841, 0.288, and 0.956, respectively. 3.3 | Comparison of characteristics between the HDP-­HDP and HDP-­Non groups (B) The HDP-­Non (6/257, 2.3%) and HDP-­HDP (18/257, 7.0%) groups did not significantly differ in maternal age, pre-­pregnancy BMI, or gestational age at delivery for either the first or second pregnancy (Table 1). The HDP-­Non and HDP-­HDP groups had similar platelet counts, hematocrit, and uric acid on day −1/0 before the first delivery. However, median antithrombin activity at day −1/0 before the (C) first delivery was lower in the HDP-­HDP (67% [59%–76%]) than in the HDP-­Non (79% [51%–103%]) group (P=0.021) (Fig. 1). Platelet counts, hematocrit, and antithrombin activity at day −1/0 before the second delivery were similar in the HDP-­HDP and HDP-­Non groups. However, uric acid at day −1/0 before the second delivery was higher in the HDP-­HDP than in the HDP-­Non group (5.8 [5.2–7.0] U/L vs 4.5 (D) [2.0–9.0] U/L) (P=0.021) (Table 3). Figure 2B shows the ROC curve of the relationship between antithrombin activity at day −1/0 before the first delivery and HDP in peripartum-­2 among women with HDP in peripartum-­2 (P=0.018). The cutoff value of antithrombin activity was 70% and the AUC was 0.824. The sensitivity, specificity, PPV, and NPV were 0.833, 0.722, 0.500, and 0.929, respectively. F I G U R E 1 Laboratory data recorded at or 1 day before the first delivery. (A) Platelet count. (B) Hematocrit. (C) Antithrombin activity. (D) Uric acid. Left, relationship between women with HDP (n=24) and women without HDP (n=233) in peripartum-­1. Right, relationship between the HDP-­HDP (n=6) and HDP-­Non (n=18) groups. 3.4 | Comparison of characteristics between the Non-­HDP and Non-­Non groups Only 3 (1.3%) of the 233 women without HDP in peripartum-­1 had HDP in peripartum-­2. Median gestational age at delivery and birthweight in the delivery were significantly lower in the Non-­HDP group than in the Non-­Non group (34 vs 38 weeks, P=0.001; and 1756 vs peripartum-­1 for the first (2184 [354–4436] g vs 2826 [420–4225] 2922 g, P=0.001). However, maternal characteristics were similar in g, P=0.002), but not the second (2710 [843–3535] g vs 2915 [1362– the two groups (Table 1). 4015] g, P=0.128) delivery (Table 2). Most laboratory parameters were similar between the Non-­ As compared with women without HDP in peripartum-­1, women HDP and Non-­Non groups at day −1/0 before the first and second with HDP in peripartum-­1 had lower platelet counts (190 [64– deliveries (Table 3). The one exception was median uric acid at day 300] × 109/mL vs 228 [67–740] × 109/mL, P=0.011), lower antithrom- −1/0 before the second delivery, which was significantly higher bin activity (74% [51%–103%] vs 89% [25%–128%], P=0.002), and in the Non-­HDP (5.4 U/L) than in the Non-­Non (4.3 U/L) group lower uric acid (5.9 [3.7–10.0] U/L vs 4.3 [1.3–8.9] U/L, P=0.004) at (P=0.047) (Table 3). day −1/0 before the first delivery (Fig. 1); however, hematocrit did not significantly differ between the two groups (Table 3). Platelet counts, hematocrit, and antithrombin activity at day −1/0 4 | DISCUSSION before the second delivery were similar between women with and those without HDP in peripartum-­1; however, uric acid at day −1 To our knowledge, this is the first study to demonstrate that women before the second delivery was significantly higher among women with HDP in their first peripartum period and low antithrom- with HDP in peripartum-­1 (5.1 [2.0–9.0] U/L vs 4.4 [1.0–8.7] U/L, bin activity (<70%) at day −1/0 before their first delivery are at P=0.004) (Table 3). increased risk of recurrent HDP in their second peripartum period. Figure 2A shows the ROC curve of the relationship between anti- The study also found that uric acid levels at day −1/0 before the thrombin activity at day −1/0 before the first delivery and HDP in first delivery were similarly high in the HDP-­HDP and HDP-­Non peripartum-­1 (P<0.001). The cutoff value for antithrombin activity was groups; therefore, high uric acid levels might be suitable for detect- 77% and the area under the curve (AUC) was 0.765. The sensitivity, ing the onset of HDP. | Morikawa ET AL. TABLE 3 5 Laboratory parameters from the first and second deliveries of the study women.a HDP in first pregnancy Parameter All women (n=24)b HDP-­HDP (n=6)c No HDP in first pregnancy HDP-­Non (n=18)d All women (n=233)e Non-­Non Non-­HDP (n=3)f (n=230)g P value <0.05 1st delivery Hematocrit, % 33.8 (28.2–38.1) 35.6 (32.8–37.3) 33.5 (28.2–38.1) 33.5 (18.8–41.6) 33.9 (32.0–34.7) 33.5 (18.8–41.6) Platelet counts, ×109/mL 190 (64–300) 190 (64–300) 228 (67–740) 254 (227–313) 228 (67–740) b vs e; d vs g AT activity, % 74 (51–103) 67 (59–76) 79 (51–103) 89 (25–128) 98 (84–102) 89 (25–128) b vs e; c vs d, f, g d vs g Uric acid, U/L 5.9 (3.7–10.0) 5.9 (5.2–9.6) 5.9 (3.7–10.0) 4.3 (1.3–8.9) 3.9 (3.8–5.9) 4.3 (1.3–8.9) b vs e c, d vs g 190 (78–95) 2nd delivery Hematocrit, % 33.4 (26.1–39.4) 34.8 (33.5–37.6) 32.1 (26.1–39.4) 33.1 (26.1–39.4) 33.4 (30.7–35.5) 33.1 (26.4–40.0) Platelet counts, ×109/mL 215 (64–422) 230 (72–610) 218 (189–314) 190 (64–319) 232 (127–422) 231 (72–610) AT activity, % 90 (70–111) 82 (73–92) 94 (70–111) 92 (44–128) 97 (86–110) 92 (44–128) Uric acid, U/L 5.1 (2.0–9.0) 5.8 (5.2–7.0) 4.5 (2.0–9.0) 4.4 (1.0–8.7) 5.4 (5.1–6.1) 4.3 (1.0–8.7) c, f vs g c vs d Abbreviations: AT, antithrombin; HDP, hypertensive disorders of pregnancy; Non, no hypertensive disorders of pregnancy. a Values are given as median (range) or number (percentage) unless stated otherwise. b all women with HDP in peripartumn-1. c women with HDP in peripartumn-1 and peripartumn-2. d women with HDP in peripartumn-1 only. e all women without HDP in peripartumn-1. f women with HDP in peripartumn-2 only. g women without HDP in either pregnancy. The study had two major strengths. First, none of the women at increased risk of HDP recurrence received prophylaxis treatment assess at day −1/0 before delivery for all pregnant women, in accordance with the study hospital's standard of care. during their pregnancies. The American College of Obstetricians A previous meta-­analysis found an increased risk of HDP recurrence and Gynecologists,15 the International Society for the Study of among 99 415 women with HELLP syndrome or delivery of small-­for-­ Hypertension in Pregnancy,16 and the UK National Institute for Health gestational-­age neonates in a first pregnancy, and the risk increased and Care Excellence17 recommend that women at increased risk of with decreasing gestational age at delivery in the first pregnancy.18 Most HDP recurrence take low-­dose aspirin every day in the peripartum obstetricians would agree that severe HDP in a first pregnancy is a pre- period to prevent the onset of HDP. Second, antithrombin activity was dictor of HDP recurrence. However, we disagree with van Oostwaard et al.'s18 comments that “among women that experience hypertension (A) (B) in pregnancy, the recurrence rate in a next pregnancy is relatively low,” because one out of five women (20.7%) experienced HDP recurrence in their analysis. Previous studies have reported recurrence rates of pre-­eclampsia varying from 6.8% to 58%,3–11 with a median of approximately 20%. In the present study, the recurrence rate of HDP and pre-­ eclampsia was 25.0% and 6.7%, respectively. In the meta-­analysis, only 9534 (9.6%) of the study women were reported to have used prophylaxis for recurrent HDP, and 950 (10.0%) of those women experienced recurrence.18 Thus, the recurrence rate in the next pregnancy would be higher if they did not experience HDP during previous pregnancy. In addition, van Oostwaard et al.18 state F I G U R E 2 ROC curve analysis. (A) ROC curve of the relationship between antithrombin (AT) activity at or 1 day before the first delivery (day −1/0) and onset of hypertensive disorders of pregnancy (HDP) in peripartum-­1. (B) ROC curve of the relationship between AT activity at day −1/0 before the first delivery and HDP in peripartum-­2 among women with HDP in peripartum-­1. that “the course of disease is milder for most women with recurrent disease; thus, reassuring data should be used for shared decision-­ making in women who consider a new pregnancy after a pregnancy that was complicated by hypertension.” In their report, the rate of stillbirth or early neonatal death was significantly lower in the second 6 | Morikawa ET AL. pregnancy than in the first pregnancy. In the present study, no women has defined pregnancy-­induced antithrombin deficiency (PIATD) as a with recurrent HDP experienced stillbirth or early neonatal death in gradual decline in antithrombin activity to 65% or less of normal lev- the second pregnancy. Thus, HDP in a subsequent pregnancy might els.23 PIATD is more likely to occur as the number of fetuses increases be milder due to both the use of prophylaxis for recurrent HDP and (approximately 1.0%, 10%, and 40% for singleton, twin, and triplet careful monitoring of the diagnosis and treatment of HDP early in the pregnancies, respectively). PIATD also increases among women with second pregnancy. HDP. In a retrospective cohort study, nearly one-­quarter of women In a recent systematic review of 68 models for predicting pre-­ eclampsia or pre-­eclampsia-­related disorders from 70 studies with with HDP had PIATD.24 Thus, the monitoring of antithrombin activity may help to predict the onset of HDP. 425 125 participants, the most frequently used predictors were medi- Previously, antithrombin was found in five ascites samples cal history, BMI, blood pressure, parity, uterine artery pulsatility index, obtained from consecutive women with both severe pre-­eclampsia and maternal age; however, the type of predictor (maternal character- and low antithrombin activity levels (≤65%) after cesarean delivery.25 istics, ultrasound markers, and/or biomarkers) was not clearly associ- Antithrombin can escape from the blood into the interstitial space ated with model discrimination.19 In the present study, maternal age among pregnant women with severe pre-­eclampsia, which would par- was found to be a predictor of HDP in the first pregnancy; however, tially explain the gradual decline in antithrombin activity observed in BMI and parity were not predictors. Furthermore, maternal age and the five pregnant women with severe pre-­eclampsia.25 Thus, women BMI were not predictors of HDP in the second pregnancy (Table 1). with both HDP and low antithrombin activity (≤65%) before delivery For multiparous women, risk factors associated with recurrent pre-­ are at increased risk of vascular endothelial dysfunction secondary to eclampsia include gestational hypertension,3 maternal age at least HDP. Therefore, we propose the following hypothesis. Pre-­eclampsia 35 years,4 previous early-­onset pre-­eclampsia,5 obesity or overweight might result from vascular endothelial dysfunction (with low anti- (BMI ≥25) before the second pregnancy,5 history of maternal cardiovas- thrombin activity) among women with a history of pre-­eclampsia. cular disease,6 and maximum diastolic blood pressure in first pregnancy.7 Thus, vascular endothelial dysfunction may recur in the second preg- Recent studies have also identified ultrasound markers and/or biomark- nancy for women with both pre-­eclampsia and low antithrombin ers that predict recurrent pre-­eclampsia, including placental maternal/ activity induced by the escape of intravascular antithrombin to the fetal vascular malperfusion lesions identified by placental pathology after extravascular space in their first pregnancy. This hypothesis will be the first delivery,8 plasma volume measured by 125I-­labeled human serum explored in future studies. albumin before the second pregnancy,9 persistent maternal cardiac dys- Women with PIATD are affected by decreased plasma volume and function after the first delivery,10 and lower fibrinogen levels or higher are more likely to develop liver dysfunction.23 Thus, low antithrom- CRP levels at the first delivery.1 In addition to those biomarkers, the pres- bin activity is a risk for HELLP syndrome or acute fatty liver in preg- ent study has found that lower antithrombin activity before the first deliv- nancy.23,24,26 Furthermore, low antithrombin activity is a risk factor for ery might also be a predictor of HDP in the second pregnancy. eclampsia.27 Therefore, vascular endothelial dysfunction in the liver Antithrombin is an important molecule for maintaining blood viscos- will result in HELLP syndrome, while that in the brain it will result in ity in the vessels and is decreased in pre-­eclampsia. Our recent study eclampsia. Therefore, pre-­eclampsia, HELLP syndrome, and eclampsia found that a cutoff of 78% antithrombin activity at the diagnosis of have the same basis as vascular endothelial dysfunction. Thus, vascular early-­onset pre-­eclampsia might be used as a predictor of delivery within endothelial dysfunction associated with antithrombin activity in preg- 7 days.20 Thus, it is clear that lower antithrombin activity among women nancy might be considered as an indicator of hypovolemia in the veins. with HDP is a predictor of poor prognosis based on the shorter inter- The present study has some limitations. First, the number of women val between pre-­eclampsia diagnosis and delivery. In a previous study with HDP in the first peripartum was small (n=24), and the number in the of women with severely low (<45%, n=6), moderately low (45%–69%, Non-­HDP group was very small (n=3). In general, however, few women n=10), and normal (>70%, n=134) antithrombin activity within 5 days of without HDP in their first pregnancy will develop HDP in their second. delivery, pregnancy-­induced hypertension (PIH), a classic criterion for Second, the study was performed at only one hospital. Women with low HDP until 2017 in Japan, was present for 16.7% (1/6), 30.0% (3/10), risk of HDP in their first pregnancy may have opted for delivery at another 21 Thus, the severity of the hospital for their second pregnancy. Third, if we could have determined decrease in antithrombin activity might be positively related to the onset and 9.0% (12/134) of women, respectively. low antithrombin activity at day −1/0 before the first delivery, we could of HDP. Antithrombin activity was also significantly and negatively cor- detect recurrent HDP during the second peripartum period. related with D-­dimer, urate, and creatinine levels.21 In a study of 792 In conclusion, the rate of HDP in the second peripartum period women with singleton pregnancy, postnatal changes in 90th percentile was higher among women with HDP in the first peripartum period. D-­dimer levels were highest for 91 women with PIH who underwent Low antithrombin activity at day −1/0 before the first delivery might cesarean delivery, followed by 371 women without PIH who underwent predict recurrent HDP in a subsequent pregnancy. emergency cesarean, and lastly 330 women without PIH women who underwent an elective cesarean.22 Thus, increased D-­dimer levels also seem to be positively correlated with the onset of HDP. AU T HO R CO NT R I B U T I O NS In previous studies, low and decreasing levels of antithrombin MM contributed to data analysis, study conception, and manuscript before delivery were used to detect the onset of HDP.23,24 A review writing. KN and KC contributed to data acquisition. TU and SK Morikawa ET AL. contributed to data interpretation. HW directed the study and contributed to manuscript revision. ACKNOWLE DG ME NTS The authors thank Enago (www.enago.jp) for their English language review. CO NFLI CTS OF I NTE RE ST The authors have no conflicts of interest. REFERENCES 1. Cunningham FG, Leveno KJ, Bloom SL. eds. Section 11. Obstetrics complications. Chapter 40 Hypertensive disorders. Terminology and diagnosis. Williams Obstetrics, 24th edn. New York, NY: McGraw-Hill Medical; 2014:728–730. 2. Ghulmiyyah L, Sibai B. Maternal mortality from preeclampsia/eclampsia. Semin Perinatol. 2012;36:56–59. 3. Brown M, Mackenzie C, Dunsmuir W, et al. Can we predict recurrence of pre-­eclampsia or gestational hypertension? BJOG. 2007;114:984–993. 4. McDonald SD, Best C, Lam K. The recurrence risk of severe de novo pre-­eclampsia in singleton pregnancies: A population-­based cohort. BJOG. 2009;116:1578–1584. 5. Mostello D, Kallogjeri D, Tungsiripat R, Leet T. Recurrence of preeclampsia: Effects of gestational age at delivery of the first pregnancy, body mass index, paternity, and interval between births. Am J Obstet Gynecol. 2008;199:55.e1–55.e7. 6. Brouwers L, van der Meiden-van RA, Savelkoul C, et al. Recurrence of pre-­eclampsia and the risk of future hypertension and cardiovascular disease: A systematic review and meta-­analysis. BJOG. 2018;125:1642–1654. 7. Bernardes TP, Mol BW, Ravelli ACJ, et al. Recurrence risk of preeclampsia in a linked population-­based cohort: Effects of first pregnancy maximum diastolic blood pressure and gestational age. Pregnancy Hypertens. 2019;15:32–36. 8. Weiner E, Mizrachi Y, Grinstein E, et al. The role of placental histopathological lesions in predicting recurrence of preeclampsia. Prenat Diagn. 2016;36:953–960. 9. Stekkinger E, Scholten RR, Heidema WM, Spaanderman ME. Recurrent pre-­eclampsia in women with metabolic syndrome and low plasma volume: A retrospective cohort study. BJOG. 2015;122:1773–1780. 10. Valensise H, Lo Presti D, Gagliardi G, et al. Persistent maternal cardiac dysfunction after preeclampsia identifies patients at risk for recurrent preeclampsia. Hypertension. 2016;67:748–753. 11. van Rijn BB, Veerbeek JH, Scholtens LC, et al. C-­reactive protein and fibrinogen levels as determinants of recurrent preeclampsia: A prospective cohort study. J Hypertension. 2014;32:408–414. | 7 12. Morikawa M, Suzuki H, Obata-Yasuoka M, et al. Association of antenatal antithrombin activity with perinatal liver dysfunction: A prospective multicenter study. J Gastroenterol Hepatol. 2017;32: 1378–1386. 13. Minakami H, Maeda T, Fujii T, et al. Guidelines for obstetrical practice in Japan: Japan Society of Obstetrics and Gynecology (JSOG) and Japan Association of Obstetricians and Gynecologists (JAOG) 2014 edition. J Obstet Gynecol Res. 2014;40:1469–1499. 14. Watanabe K, Naruse K, Tanaka K, Metoki H, Suzuki Y. Outline of definition and classification of “pregnancy induced hypertension (PIH)”. Hypertens Res Pregnancy. 2013;1:3–4. 15. Committee on Obstetric Practice. Committee opinion No. 638: First-­trimester risk assessment for early-­onset preeclampsia. Obstet Gynecol. 2015;126:e25–e27. 16. Tranquilli AL, Dekker G, Magee L, et al. The classification, diagnosis and management of the hypertensive disorders of pregnancy: A revised statement from the ISSHP. Pregnancy Hypertens. 2014;4:97–104. 17. National Collaborating Centre for Women's and Children's Health. Hypertension in pregnancy: the management of hypertensive disorders during pregnancy. (NICE Clinical Guideline, January 2011) https://www.nice.org.uk/guidance/cg107?unlid=373304423201622 8134435. Accessed October 1, 2019. 18. van Oostwaard MF, Langenveld J, Schuit E, et al. Recurrence of hypertensive disorders of pregnancy: An individual patient data metaanalysis. Am J Obstet Gynecol. 2015;212:624.e1–624.e17. 19. De Kat AC, Hirst J, Woodward M, Kennedy S, Peters SA. Prediction models for preeclampsia: A systematic review. Pregnancy Hypertens. 2019;16:48–66. 20. Morikawa M, Umazume T, Hosokawa-Miyanishi A, et al. Relationship between antithrombin activity and interval from diagnosis to delivery among pregnant women with early-­onset pre-­eclampsia. Int J Gynecol Obstet. 2019;145:62–69. 21. Yamada T, Ishikawa S, Kataoka S, et al. Coagulation/fibrinolysis and laboratory characteristics of pregnant women with severely depressed antithrombin activity. Hypertens Pregnancy. 2013;32:235–244. 22. Morikawa M, Yamada T, Yamada T, et al. Changes in D-­dimer levels after cesarean section in women with singleton and twin pregnancies. Thromb Res. 2011;128:e33–e38. 23. Minakami H, Morikawa M, Yamada T, Yamada T. Candidates for the determination of antithrombin activity in pregnant women. J Perinat Med. 2011;39:369–374. 24. Morikawa M, Yamada T, Yamada T, et al. Pregnancy-­induced antithrombin deficiency. J Perinat Med. 2010;38:379–385. 25. Morikawa M, Yamada T, Yamada T, et al. Evidence of the escape of antithrombin from the blood into the interstitial space in pregnant women. J Perinat Med. 2010;38:613–615. 26. Morikawa M, Kawabata K, Kato-Hirayama E, et al. Liver dysfunction in women with pregnancy-­induced antithrombin deficiency. J Obstet Gynecol Res. 2017;43:257–264. 27. Yamada T, Kuwata T, Matsuda H, et al. Risk factors of eclampsia other than hypertension: Pregnancy-­induced antithrombin deficiency and extraordinary weight gain. Hypertens Pregnancy. 2012;31:268–277.