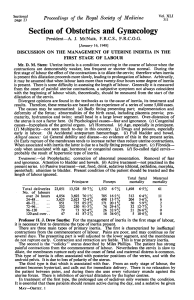
European Journal of Obstetrics & Gynecology and Reproductive Biology 95 (2001) 149±153 Uterine electrical activity as predictor of preterm birth in women with preterm contractions Ivan Verdenik*, Marjan Pajntar, Brane LeskosÏek Department of Obstetrics & Gynecology, University Medical Center, Ljubljana, Slovenia Accepted 14 June 2000 Abstract Objective: To estimate the risk of preterm birth in women admitted to the tertiary maternity hospital for preterm contractions by measuring electrical uterine activity. Study design: The study included 47 patients with contractions between the 25th and 35th week of gestation and additional risk factors for preterm delivery. Uterine electrical activity was recorded using bipolar electrodes placed on the abdominal surface. A logistic model with the electromyographic and obstetric data was built, preterm delivery before 37th week of gestation being the outcome measure. Results: Seventeen patients (36%) delivered before term. Logistic regression model suggested only the intensity of electrical uterine activity and woman's body weight to be signi®cant predictors of preterm delivery, with high values related to preterm birth. They predict preterm delivery with the sensitivity of 47% and speci®city of 90%. Conclusion: We propose uterine EMG as a simple, non-invasive means to estimate the risk of preterm birth in a high-risk population with multiple risk factors present. # 2001 Elsevier Science Ireland Ltd. All rights reserved. Keywords: Preterm birth; Uterine electrical activity; Preterm contractions 1. Introduction 2. Materials and methods Preterm birth is the single most important contributor to infant morbidity and mortality [1]. Although the majority of risk factors for preterm birth have been identi®ed [1±3], the prediction models exhibit a relatively poor performance. On the other hand, the effectiveness of tocolytic agents depends on early introduction of therapy [1], therefore, timely recognition of the process leading to active labor is of prime importance. Uterine contractions are a necessary, but not suf®cient condition to recognize the onset of labor [4]. Monitoring of uterine contractions [5] does not help to identify patients who are likely to deliver prematurely. Over the last 10 years, uterine and cervical electrical activity have become the object of many research studies [6±8], offering a better insight into the pregnant uterus and the process of labor. Electrical activity of uterine muscles precedes mechanical activity [6,8,9] and is together with cervical electrical activity [7,10] related to initiation of labor [11±13]. Therefore, the purpose of this study was to attempt to de®ne factors that could identify the women in the high-risk population in danger to deliver before term. This study was approved by the National Ethical Committee, and all patients were enrolled in the trial after giving informed consent. The enrolment took place in the main tertiary center in the Republic of Slovenia between May 1996 and June 1997. The patients came to hospital for uterine contractions in the third trimester of pregnancy. When contractions were con®rmed by tocography or when the obstetrician judged the mother should be hospitalized for closer monitoring (possibly also for additional risk factors) she was admitted to the obstetric ward, where there they were recruited for the study. Only about 10% of the approached patients refused to participate. The exclusion criteria were severe obstetric pathology and cervical dilatation over 3 cm (labor in progress). All together, 49 patients were enrolled in the study. For the analysis we also excluded two patients with induced preterm labor, therefore, data are based on the remaining 47 patients. Before any medication for uterine relaxation was given, recording of the electrical uterine activity was done. The time elapsed from the initial check to the recording was usually a few hours. All the patients were white. The mean gestational age, estimated by the last menstrual period (LMP) or ultrasound examination was 30.0 weeks (range 25±35 weeks). The average maternal age was 26.95.2 * Corresponding author. Fax: 386-1-4397590. E-mail address: [email protected] (I. Verdenik). 0301-2115/01/$ ± see front matter # 2001 Elsevier Science Ireland Ltd. All rights reserved. PII: S 0 3 0 1 - 2 1 1 5 ( 0 0 ) 0 0 4 1 8 - 8 150 I. Verdenik et al. / European Journal of Obstetrics & Gynecology and Reproductive Biology 95 (2001) 149±153 years; 47% were nulliparous; 45% had abortion (either spontaneous or induced) in their medical history; 4% had conisation; 4% were smokers; as much as 34% had preterm delivery in their obstetric history. At the time of recording the electrical activity, only 23.4% still had uterine contractions at a rate of at least 1 per 10 min. Medical intervention went on regardless of the recording of uterine electrical activity. Different uterine relaxation drugs were given according to the doctor in charge of a particular patient: 17% (eight patients) received tocolytic drugs (Mg sulfate, Ritodrine), 49% spasmolytics (butyl scopolamine). Simultaneously, 15% received dexamethasone for fetal lung maturation. The sites of electrode attachment were carefully cleansed and brushed with a ®ne abrasive paper and treated with the electrode gel. Bipolar silver±silver-chloride electrodes (in vivo Metrics Inc., USA) 5 mm in diameter were applied to the abdominal wall by the adhesive tape 7 cm apart, approximately 12 cm above the symphysis. The reference electrode was placed on the patient's right thigh. The electromyographic activity was ampli®ed, acquired and digitized using DAS-8/PGA (Keithley Metrabyte Co., Taunton, MA) and PC. The data were bandpass ®ltered in the 0.1±4 Hz frequency range. The sampling frequency was set at 20 Hz. At the same time, cardiotocographic monitoring was applied (Hewlett Packard 8030; Hewlett-Packard Co., Cupertino, CA), and digitized and stored simultaneously. The recording lasted 30 min. The root mean square (RMS) value of the signal is a standard measure to quantify signals [14]. It is equivalent to the intensity of constant voltage applied to a pure resistance and is used to assess the intensity of electrical activity. As the uterine activity is changing with the time, it is important to analyze also in the frequency domain [15]. As the second quantitative measure of frequency of uterine electrical activity, the median frequency of power spectra was chosen. The signal analysis was done using MATLAB software package (MathWorks Inc., Natick, MA), using supplied routines, adapted for the task at hand. Recorded sequences were analyzed en-bloc, because the identi®cation of bursts in this stage of gestation is usually impossible. Fig. 1. illustrates signal processing procedure, with raw EMG signal on upper Fig. 1. Top trace: raw uterine EMG signal as detected transabdominally. Second trace: intrauterine pressure as detected with cardiotocograph (contractions). Third trace: RMS value calculated from the filtered uterine EMG signal. Horizontal line represents mean RMS over the observed period (30 min). Bottom trace: median frequency of the uterine EMG. Horizontal line represents mean MF in the observed period. I. Verdenik et al. / European Journal of Obstetrics & Gynecology and Reproductive Biology 95 (2001) 149±153 151 Table 1 Comparition of groupsa Maternal age (years) Body weight (kg) Smoking Conization Primiparous Previous preterm delivery Previous abortion Gestational age at admission (weeks) Uterine contractions Median frequency (Hz) RMS value (mV) Birthweight (g) Spasmolytics Tocolytics a Preterm group (N17) Term group (N30) Statistical significance P 27.35.5 72.77.30 1 (6%) 2 (12%) 9 (53%) 5 (29%) 7 (41%) 30.13.2 3 (18%) 0.360.068 17.57.78 2200747 9 (53%) 3 (18%) 26.75.1 67.88.42 1 (3%) 0 13 (43%) 11 (37%) 14 (47%) 29.92.8 8 (27%) 0.370.049 12.26.25 3069460 14 (47%) 5 (17%) NS NS NS NS NS NS NS NS NS NS <0.05 <0.05 NS NS Numbers are meanS.D., or N with percents. Statistical significance was obtained by t-test or w2-test as appropriate for given variable. trace, intrauterine pressure (contractions) on second, RMS on the third and median frequency on the bottom trace. Of the 47 patients in the study, 30 (63.8%) managed to complete 37 weeks of pregnancy, whereas the remaining 17 (36.2%) had a preterm delivery. The average prolongation of pregnancy from the time of recording to delivery was 47 days, range from 1 to 113 days. None of the newborns died. Three patients in the term group had induced labor, in others the onset of labor was spontaneous. Of the 47, 13 labors (28%) had to be ended by a cesarean delivery. The general data on patients and the two parameters computed from the recorded uterine electrical activity were entered into the statistical package SPSS v8.01 (SPSS Inc., Chicago IL). Pearson correlation coef®cients were ®rst computed to explore univariate relationship between the parameters. For building the logistic regression model, a forward stepwise method was used, where the variables describing the patient's general condition and medical history together with the parameters of uterine electrical activity were proposed to the model. The ®rst group of variables consisted of the patient age (years), weight at admission (kg), smoking status (smoking/non-smoking), gynecological history of uterine anomalies, conisation, parity, previous abortions (either spontaneous or induced), previous preterm deliveries, gestational week at admission, membrane status, presence of contractions at arrival to the obstetric ward (at least one per 10 min, con®rmed by tocography), treatment with spasmolytics and/or tocolytics. Of the electrical myographic parameters, RMS value and median frequency were used. Table 1 shows the values of variables for both groups. Univariate tests show that statistically signi®cant were only lower birthweight and higher RMS value of the uterine EMG in the preterm group. Table 2 con®rms independence of electrical parameters of weight, age, parity and gestational age. Asterisk denotes Spearman (non-parametric) correlation, as parity does not follow normal distribution, and other r's are Pearson correlation coef®cients. No statisticaly signi®cant correlation was found. On the other hand, the correlation between two electrical parameters, namely the RMS value and median frequency of uterine electrical activity, was signi®cant and negative (rÿ0.435; P0.002). The results of the stepwise logistic regression are shown in Table 3. From the 14 independent variables proposed initially to the procedure, only two of them, namely the RMS value and weight of the woman, ful®lled the conditions necessary to be entered into the model (probability of F to enter was set at 0.05). The procedure was executed with term delivery as the dependent variable. Resulting logistic model therefore, consists of only two terms. The accuracy of prediction of preterm delivery with the above described logistic model is given in Table 4. Standard measures of predictive parameters are therefore: sensitivity 47.1%, speci®city 90.0%, positive predictive value 72.7% and negative predictive value 75.0%. Table 2 Correlation of the parameters of the electrical uterine activity to age, weight, parity and gestational age of the patienta 3. Results Of the electrical myographic parameters, the RMS value and median frequency were used. The mean RMS value observed was 14.2 mV (S.D. 7.2); the mean recorded median frequency was 0.36 Hz (S.D. 0.06). Both were normally distributed. Age Weight Parity Gestational age RMS value of the uterine electrical activity Median frequency of the uterine electrical activity rÿ0.053 (0.723) r0.048 (0.750) rÿ0.170 (0.254) r0.139 (0.353) r0.142 (0.342) r0.169 (0.256) r0.312 (0.066) rÿ0.234 (0.113) a r: Pearson correlation coefficient; r: Spearman correlation coefficient; statistical significance P is given in the parenthesis. 152 I. Verdenik et al. / European Journal of Obstetrics & Gynecology and Reproductive Biology 95 (2001) 149±153 Table 3 Results of stepwise logistic regression with term delivery as the dependent variable Variables in the model RMS value Body weight Ba S.E. (B) Sig. R2b ÿ0.1189 ÿ0.0842 0.0535 0.0445 0.026 0.0586 0.048 0.026 Variables not in the model Conization Age of the women Previous preterm delivery Median frequency Uterine anomalies Previous abortion Parity Gestational age Uterine contractions Spasmolytics Tocolytics Smoking 0.2665 0.3764 0.4321 0.4766 0.5142 0.6110 0.6182 0.6465 0.7401 0.7486 0.9084 0.9711 a B: regression coefficient; S.E.: standard error; Sig.: statistical significance. b 2 R : variation of preterm delivery explained by particular factor. Table 4 Predicted and actual outcome of pregnancy Actual preterm delivery Actual term delivery Predicted preterm delivery by the logistic model Predicted term delivery by the logistic model 8 (True positives) 3 (False positive) 9 (False negative) 27 (True negative) 4. Comment The patient's individual perception of uterine contractions varies too much to be useful for predicting the closeness to delivery. It depends on sensitivity of the woman and her previous obstetric experiences. At admission to the ward, contractions were recorded in only 23.4% of the patients, although they all came to the maternity hospital for preterm contractions. In our institution, women who come for uterine contractions in the third trimester of pregnancy, routinely undergo cardiotocography. According to the fetal and maternal condition, course of pregnancy and medical history, the decision is made whether she should be hospitalized or not. To obtain a better insight into the uterine activity leading to preterm delivery, some authors investigated continuous monitoring of uterine contractions. As a result, home uterine monitoring study [5] revealed that everyday monitoring of contractions with electronic devices is not linked to earlier diagnosis of preterm labor. We believe that the prediction of preterm labor was not successful because of weak and irregular mechanical uterine activity in pregnancy. Therefore, we decided to measure the parameter which underlies contractility, i.e. the electrical uterine activity. As the time of delivery approaches, uterine electrical activity becomes more and more synchronous, acting towards expulsion of the fetus. This synchronous activity is known as `uterine contractions' in mechanical sense and as `signal bursts' in electrical sense. However, during normal pregnancy until 36th week, there is almost no synergy of muscular ®bers, and contractions or bursts can only seldom be detected [8]. In our previous study [10] we have found that during labor the activity between two bursts is related to the course of labor. Therefore, the analysis of signals during bursts only is not suf®cient. By analyzing the overall signal in certain (we chose 30 min) time period it is possible to get insight into the preparedness of the uterus for labor, even in the state without contractions. Our study group patients were at high risk for preterm delivery; as much as 34% of them had (at least) one before, and almost a half had abortions in their medical history. The therapy for this group was administered according to everyday care, regardless of our study; 17% of patients received tocolytics, 49% spasmolytics, and bedrest and observation was prescribed in the remaining ones. The distribution of drugs was similar in those who delivered before term and in those who delivered at term. All recordings we made, were done in 25th±35th week of pregnancy, with majority around 30th week. Therefore, the conclusions we reached are valid for this gestational age only. The correlation between EMG parameters and gestational age shows that with duration of pregnancy the frequency contents of electrical activity becomes lower, which is expressed as lower median frequency of uterine electrical activity. At the same time the RMS value does not statistically signi®cantly correlate with gestational age. These results are different from those of Buhimschi and coworkers [13,15], who found that the frequency power spectrum moves higher as the time of labor approaches. This difference occurred because we measured the complete 30 min interval and not only bursts, which are by and large nonexistent in this stage of gestation. The second source of differences could be signal ®ltering; namely, Buhimschi and Gar®eld [13] used signal bandpass 0.3±50 Hz, whereas we chose the 0.1±4 Hz frequency band. The reasoning behind this decision was the report published by Devedeaux et al. [6], who found signi®cant part of power spectrum density as low as 0.1 Hz. Also, at frequencies close to 50 Hz (60 Hz in US), electromagnetic noise could signi®cantly contaminate the signal. We have found that weight, age and parity of the patient do not correlate with the recorded electrical activity. Predictive logistic regression model shows the most important risk factor for preterm delivery to be high RMS value followed by the weight of the woman. We believe that with the closeness to delivery the electrical activity of the uterus becomes more vigorous, despite yet weak and/or irregular contractions (mechanical activity measured by tocodynamometer). Regarding body weight we found a I. Verdenik et al. / European Journal of Obstetrics & Gynecology and Reproductive Biology 95 (2001) 149±153 positive correlation between body weight and risk for preterm delivery, as was also found by Carmichael et al. [16]. Data on weight were obtained at the time of measurement. For more accurate analysis, one should also take into account prepregnancy weight, height, body mass index, etc. but that was beyond the scope of this study. It is surprising that all other factors, which are usually considered risk factors for preterm delivery, did not contribute signi®cantly and were therefore not entered into the model. We believe that this is because almost all of the patients had one or more risk factors for preterm birth present, and 17 of them (36.2%) delivered before term. Strong correlation between the median frequency of the uterine electrical activity and gestational age would also suggest the importance of median frequency for preterm delivery. However, it seems that during pregnancy the median frequency changes (decreases) with gestation in linear fashion, whereas the RMS value changes only a few days before the true labor begins. A higher RMS value of the uterine electrical activity in the patients who delivered before term suggests that this could be a sign of physiological characteristics of women prone to preterm labor, independent of other well-known risk factors. This is an important ®nding because the RMS value of the electrical uterine activity is neither signi®cantly related to the duration of gestation, nor to the time left to delivery. It is a static marker, denoting the woman's risk for preterm delivery, independent of other possible causes. The analysis of electrical uterine activity is therefore a promising method for evaluating evolution of uterine contractility, determining preparedness of uterus for labor and identifying patients at risk for preterm delivery. References [1] Mclean M, Walters AWW, Smith R. Prediction and early diagnosis of preterm labour: a critical review. Obstet Gynecol Surv 1993;48:209± 25. 153 [2] Iams JD, Goldenberg RL, Mercer BM, Moawad A, Thom E, Meis, PJ, et al. The preterm prediction study: reccurence risk of spontaneous preterm birth. Am J Obstet Gynecol 1998;178:1035±40. [3] Bakketeig LS, Bergsjú P, The epidemiology of preterm birth. In: Kurjak A, editors. The textbook of perinatology. Parthenon Publishing, 1998. p. 1331±6. [4] Hueston WJ. Preterm contractions in community settings. II. Predicting preterm birth in women with preterm contractions. Obstet Gynecol 1998;92:43±6. [5] Devoe LD, Artal R, Goodwin TM, Weiner C, Witter F, McGregor J, et al. A multicenter randomized controlled trial of home uterine monitoring: active versus sham device. Am J Obstet Gynecol 1995;1120±7. [6] Devedeux D, Marque C, Mansour S, Germain G, Duchene J. Uterine electromyography: a critical review. Am J Obstet Gynecol 1993;169:1636±53. [7] Pajntar M, Roskar E, Rudel D. Electromyographic observation of the human cervix during labor. Am J Obstet Gynecol 1987;156:691±7. [8] Buhimschi C, Boyle MB, Garfield RE. Electrical activity of the human uterus during pregnancy as recorded from the abdominal surface. Obstet Gynecol 1997;90:102±11. [9] Shafik A. Electrohysterogram: study of the electromechanical activity of the uterus in humans. Eur J Obstet Gynecol Reprod Biol 1997;73:85±9. [10] Pajntar M, Verdenik I, Pusenjak S, Rudel D, Leskosek B. Activity of smooth muscles in human cervix and uterus. Eur J Obstet Gynecol Reprod Biol 1998;79:199±204. [11] Marque C, Gondry J, Rossi J, Baaklini N, Duchene J. Surveillance des grossesses a risque par electromyographie uterine. RBM 1995;17:25±31. [12] Gondry J, Marque C, Duchene J, Cabrol D. Electrohysterography during pregnancy: preliminary report. Biomed Instrum Technol 1993;27:318±24. [13] Buhimschi C, Garfield RE. Uterine contractility as assessed by the abdominal surface recording of EMG activity in rats during pregnancy. Am J Obstet Gynecol 1996;174:744±53. [14] Ramondt J, van Kooten C, Verhoeff A, Wallenburg HCS. Computer analysis of mechanical and electrical uterine activity. Med Biol Eng Comput 1986;24:351±5. [15] Buchimschi C, Boyle MB, Saade GR, Garfield RE. Uterine activity during pregnancy and labor assessed by simultaneous recordings from the myometrium and abdominal surface in the rat. Am J Obstet Gynecol 1998;811±22. [16] Carmichael S, Abrams B, Selvin S. The association of pattern of maternal weight gain with length of gestation and risk of spontaneous preterm delivery. Paediatr Perinat Epidemiol 1997;11(4):392±406.