Uploaded by
common.user58599
Shoulder Instability: Classification, Diagnosis, and Management
advertisement

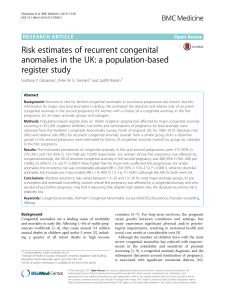
Mini-synqmdum: the sbuider (iv) Shoulder Instability R. J. Hawkins, S. R. Saddemi - Introduction riorly, with anterior instability historically being the most common. The shoulder may also be unstable in more than one direction, termed multi-directional instability. Inferior and anterior along with inferior and posterior are the most common multi-directional instabilities, but instability in all three directions may occur. In order to be multi-directional, symptomatic inferior instability should be present, in addition to instability in at least one other direction. The degree of instability is also an important component of the classification. A dislocation is a complete loss of the normal gleno-humeral articula- Shoulder instability has been a problem for treating physicians for hundreds of years. Hippocrates, the father of medicine, wrote detailed descriptions of shoulder anatomy, dislocations and their treatment. The concepts regarding the diagnosis, classification, and management of shoulder instability have evolved greatly over the years. The evolution is not yet complete as today’s shoulder experts are still debating the best ways to diagnose and classify shoulder instabilities and the optimal ways to treat them. The latest controversial area in the management of shoulder instabilities relates to arthroscopically assisted stabilization for anterior instability which may play a larger role in the management of shoulder instability in the future. The purpose of this report is to review the concepts of shoulder instability as they relate to classification, diagnosis, and management. Table I Multi-directional Anterior-Inferior Posterior-Inferior Anterior-Posterior-Inferior Classification The classification of shoulder instability is based on many factors such as direction, degree, chronology, etiology, and volition (Table). All of these factors can play a role in the classification of a particular patient’s instability. The direction in which a should is unstable is an important aspect of the classification. Uni-directional instabilities of the shoulder occur anteriorly or poste- Current Orthopaedrcs (1990) 4,242-252 II Degree Dislocation Subluxation III Chronolog> Acute Chronic Recurrent Locked IV Etiology Traumatic Atraumatic Hyperlaxity Overuse-Acquired Hyperlaxity and Overuse R. J. Hawkins MD, FRCS, The University of Western Ontario, University Hospital, 339 Windermere Road, London, Ontario, Canada N6A 5A5. S. R. Saddemi MD, Director of Sports Medicine, Medical College of Ohio. Toledo, Ohio 43699, N5A. 0 1990 Langman Group UK Ltd Direction Uni-directional Anterior Posterior Inferior V Volition Voluntary Involuntary Positional 0268~890:90/ooO4 242 0242/$,0 00 SHOLJLDER INSTABILITY tion. while a subluxation is a partial loss of glenohumeral articulation. Dislocations and subluxations may occur in any direction and both may occur at different times in the same patient. The chronology or the timing of the dislocation or subluxation is also LI part of the classification. The instability ma\ be acute or chronic; if chronic it may be locked or recurrent. The etiology of the instability is important because it implies different management. A dislocation or subluxation rn;ly be traumatic or atraumatic. Traumatic dislocations occur as a result of 3 significant injury. Atraumatic dislocations occur in two situations : in those with hypermobility and hyperlaxity of the shoulder, and in those who overuse their shoulders repeatedly, especially in the overhead position. Both factors. hypermobility and overuse, may contribute to an atr,iumatic dislocation. These individuals are particularly prone to multi-directional instability. The volition ot‘the dislocation is the final component of the classification. A dislocation is either voluntary or involuntary. A voluntary dislocation occurs when the indrvidual intentionally. willfully dislocates his or her shoulder with muscular contraction. An involuntary dislocation occurs without any overt attempt on the part of the patient todo so. Involuntary dislocations may be positional. meaning that the dislocation occurs when the patient places his arm in a certain position. Generally positional dislocations are involuntary, occurring when the patient positions his arm for ;I particular functron or activity. Positional dislocations may, however. become voluntary over time, if the patient places the arm in ;I certain position merely to cause the dislocation. Certainly voluntary and involuntary episodes may coexist in the hvme patient. Voluntary dislocators occasionally require psychiatric evaluation in addition to treatment of their shoulder. Matsen has introduced acronyms to broadly classify two groups of patients with shoulder instability.’ Patients with ‘Traumatic shoulder instability often have a Unilateral problem, a Bankart lesion, and usually require Surgery for optimal management’ terms ‘TUBS.’ (Traumatic, Unilateral, Bankart, Surgery).: On the (Ither hand. patients with an ‘Atraumatlc initial Injury may have multi-directional instability. often have bilateral shoulder instability and usually respond to a specific rehabilitation program. Should surgery became necessary in this patient, an infcrlor capsular shift is the appropriate procedure.’ This is the ‘AMBRI’ group (Atraumatic, Multi-directional. Bilateral. Rehabilitation, Inferior Capsular Shift). . In reviewing the classification ue must remember that it ih important to know the direction, degree. chronology, etiology, and volition of the instability, For example, one who sustains an anterior dislocation while making an arm tackle playing football has an ‘Acute Traumatic Anterior Dislocation.‘ if that individual has several subsequent episodes of instability, he has ‘Chronic Recurrent Anterior Instability’. The 243 instability may be further classified bq the degree depending on whether dislocations and,‘or subluxations occur. The classification is important because it implies which management is most effective. Anatomy and Biomechanics The gleno-humeral joint is dislocated more frequently than any other joint in the body. This is not surprising in view ot’ the great mobility present at this joint, which lives in a milieu consisting of ;I trade-off between stability and mobility. ‘The stability ofthe gleno-humeral joint is dependent on the intergrated function of the bony architecture, the labrum. capsule. gleno-humeral ligaments. dynamic muhclc function, and an internal pressure gradient compared to atmospheric pressure The bony architecture of‘ the shoulder does not contribute much to its stability. The glenoid is relati\elq flat with a radius of curvature less than half thar of the humcral head, and cover\ onl) about 15 33”,, of the humeral head. Sidles compared the glenohumeral articulation to a ‘golf ball on a tee‘. referring to 11s l,ick ctf inherent stability. The glenold labrum increases the radius ot‘ cur\‘ature and deepens the gtenoid. thus making it more concentric with the humeral head. The tabrum is also important as it series as the attachment site for the glens-humeral ligaments. T-he gleno-humeral ligaments control passive and dyn,lmlc stability of the shoulder. The superior. middle and inferior gleno-humeral ligaments act in concert pro\ iding stability. The ligaments function by tightening at the extremes of motion to limit further translation of the humerus preventing a suhtuxation or dislocation. The inferior gteno-humeral ligament with its anterior and posterior bands is the prime stabilizer of the shoulder, resisting anterior. posterior and mfcrior translation. The superior gleno-humeral ligament is l’elt to have little function in pr-eventing anterior 1nstabillty. but does restraIn lnlcrior and postcarior translation. The middle gleno-hunlrral ligamen! act5 as a secondary restraint to anterior- translation. and al40 functions to limit external rotation ‘it 45 of abduction. The most vulnerable positlon for the shouider is elevation above the horirontal. especially as it is forced into excessive extern;tl rotation and extelision. It is at this position that the inferior gtenohumcral ligament tightens. acting as :I check-rein to limit further external rotation and pre\‘ent anterio instability. Ligament cutting studies have shown that cutting all of the posterior ligamentous structures alone did not allow a posterior dislocation. Dislocation posteriorly did not occur until the anterior- superior capsule and superior gleno-humeral ligament *ere cllt from the 12 to 3 o’clock position ;lntcriorly. The authclrs concluded that the shoulder acts as ;I ‘circle’. in th,lt tight lor loose ligaments on one \ide ot. the joint may %tffect translation not only on that sl&. but alxo on the opposite side of theJoint. 244 CURRENT ORTHOPAEDICS-MINI-SYMPOSIUM: Dynamic stability of the shoulder is provided in large part by the muscles crossing the joint. Muscle contraction increases joint compression, thus increasing stiffness and decreasing translation. The rotator cuff muscles, because of their origins and insertions, are well positioned to resist subluxating forces by creating joint compression. They act concentrically on one side to provide movement and eccentrically on the opposite side to maintain stability. The position of the glenoid is also important in gleno-humeral stability, making scapular function important. The trapezius and serratus anterior are the primary movers of the scapula and should be assessed when evaluating glenohumeral stability. SHOULDER m, Normal attachment of 0.5 cm avulsion of labrum and capsule from glenoid rim (mild). NPE I Bankart Lesion 1.0 cm avulsion of labrum and capsule (moderately severe) NPE II Bankan Lesion Pathophysiology With knowledge of normal gleno-humeral anatomy, biomechanics, and the factors which contribute to normal gleno-humeral stability, we can better understand the pathophysiology of shoulder instability. Dysplasia or damage to the humeral head or glenoid, loss of integrity of the capsular-labral-ligamentous complex, or muscle dysfunction may all contribute to instability. The ‘essential’ lesion is that pathologic lesion responsible for perpetuating the recurrent instability. There may commonly be more than one ‘essential’ lesion. Rowe’ categorized the various pathologic lesions into three areas: (1) Capsular lesions. (2) Muscular lesions, and (3) Bony lesions. There are three capsular lesions : (1) Rupture of the capsule and labrum from the rim of the glenoid (the Bankart lesion), (2) Rupture of the capsule from the humeral neck, and (3) Excessive laxity of the capsule secondary to repeated injury (Fig. 1). Most investigators agree that the most common lesion accounting for recurrent anterior dislocations and subluxations of the shoulder is an avulsion of the labrum and capsule from the glenoid rim, better ANATOMICAL LESIONS I \ “Reverse” Hill-Sach’s (posterior dislocation) Hill-Sachs lesion Bankart lesion Anatomic variatibns of the glenoid ( THE \ Fig. l-Reprinted from: Rowe, C. The Shoulder. New York: Churchill Livingstone, 1988. 1.5 cm + avulsion of capsule. The labrum may be difficult to identify, as it is either worn away or absorbed into the capsule. Glenoid rim is eburnated (severe). TYPE Ill Bankart Lesion .\ TYPE IV Fracture of Anterior Glenoid rim ‘. Different degrees of fracture of the glenoid rim may occur. The avulsed rim is usually enmeshed in the capsule. -81) Fig. 2-Reprinted from: Rowe, C. The Shoulder. New York: Churchill Livingstone, 1988. known as ‘the Bankart lesion’ (Fig. 2). Avulsion of the capsule from the glenoid rim was noted by Caird in 1887, then by Broca and Hartman in 1890, and Perthes in 1906. It was later popularized by Bankart in 1923.” In Rowe’s follow-up series a Bankart lesion was found in 85% with traumatic recurrent anterior dislocation,l in 64% with recurrent anterior subluxationqs and in 84”,/,of those operated upon for previous failed anterior surgical procedures.h Excessive capsular laxity may be present alone or in conjunction with a Bankart lesion, often contributing to the instability. Rowe found abnormal capsular redundancy in 28% of those with traumatic recurrent anterior dislocations, in 26% of those with recurrent anterior subluxations, in 86”/0 of those with previous failed anterior surgical procedures, and in loo’?/, of those with voluntary subluxation.7 A recent presentation by Uribe at the American Orthopaedic Society for Sports Medicine in 1989 documented the arthroscopic pathology in 45 patients with an acute traumatic primary anterior dislocation. These patients were placed into one of three groups based on the intra-articular pathology and the examination under anesthesia. Type I included II”, of the patients who were felt to have stable shoulders under SHOULDER ______.~ anesthesia, minimal hemarthrosis and had a capsular tear only, Type 1 included 34”, of the patients with increased anterior translation indicative of anterior instability, a more obvious hemarthrosis and separation of the glenoid labrum. Type 3 was by far the largest group including 63”, of the patients. They had gross anterior instability with complete avulsion of the anterior labrum. Muscle lesions are a much less frequent and more poorly understood cause of shoulder instability. In Rowe’s series of I58 shoulders operated on fo1 recurrent anterior dislocation, the subscapularis was considered normal in 83”,, ‘attenuated’or’inadequate‘ in IO”,,. and ruptured in 7°r,.J Although certainly more difficult to document. a certain percentage of patients with recurrent anterior instability also ha\-e pathology of the rotator tuft: primarily the supraspinatus. We know that a strong rotator cuff is important in providing dynamic gleno-humeral stability, and Jobe has introduced the concept ofcoexistence of instability and impingement. so we must be much more critical in our analysis of the rotator cuff and its function when evaluating gleno-humeral instability. We also must be aware ot‘the high incidence of acute rotator cuff tears in those patients who are over 40 years of age at the time of an acute traumatic anterior dislocation. Rowe also noted another ‘muscle lesion’ in a series of 37 patients operated on for recurrent anterior subluxation.< An enlargement of the normal seam between the subscapularis and supraspinatus tendons (i.e. ‘the rotator interval’) was seen in 20 of the 37 shoulders. This may represent loss of the normal suspensory mechanism and may contribute to anterior instability. Bon) lesions may also contribute to shoulder instability. A bony defect of the humeral head to glenoid may be one of the ‘essential’ lesions contributing to gleno-humeral instability. The Hill-Sachs lesion. an osteochondral compression defect of the posterior humeral head. is produced by impaction of the humeral head against the glenoid rim at the time of dislocation. Hill-Sachs lesions of varying degrees often exist. Rowe found Hill-Sachs lesions in 77”, of 143 traumatic dislocations,’ in 40°, of those with recurrent subluxation.’ and in 76”” of failed surgical repairs.” Glenoid rim damage may also contribute to instability. Rowe found glenoid rim damage in 73O, of those with traumatic recurrent anterior dislocations,l in 45”, of those with recurrent anterior subluxation.i and in none of the \Toluntary dislocators or subluxatars. _ Diagnosis and Management Instabilities Anterior glmo-hunwml of Specific instahiiit.~~ Acute traumatic anterior dislocations. An acute anterior dislocation is by far the most common form of acute shoulder instability. The overall incidence of shoulder dislocations is estimated to be between 1 and 3”0 ot INST.ABII.ITY ____ ‘45 the population” with anterior dislocations accounting for about 98”” of these.” Dislocations are approximately twice as common in males than females.” The diagnosis is made by an appropriate histor!. physical examination and radiographic evaluation. 7he usual patient is a male who injures his shoulder in an athletic event. The mechanism of in.jury is an extremely important part of the history, as It is often the best clue as to which direction the shoulder dislocated. Indirect force to the shoulder, usually from a direct force applied to the arm, which results in excessive abduction, extension and external rotation is the usual mechanism of injury. These forces cause attenuation and disruption of the static and dynamic anterior stabilizers of the joint, and the humeral head dislc)cates anteriorlv. To summarize. the important part\ of the history are the position of the arm and the degree and position of the applied force at the time of the injury. The patient may also be able to relate in which direction the shoulder dislocated. whether or not paresthesias were present. and the details of reduction following the injury. Atter obtaining a thorough history, the physical examination typically reveals a patient with a very painiul. tender shoulder. There is muscle spasm about the shoulder and inspection reveals ;I hollow posterior]! beneath the acromion. The arm is generally held across the abdomen and the patient is unable to full> rotate or abduct the arm. The physician should be sure to document axillary nerve function since it may he injured at the time of dislocation. Radiographs 01‘the injured shoulder in t&o planes 90 to one another are essential. We recommend a true anterior-posterior (AP) view ofthe shoulder and a true axillary X-ray. A true axillary X-ray often cannot be obtained, and with an acute anterior dislocation the AP view alone combined with a history and physical will document the dislocation. In this case the AP and axillary view\ should be obtained after reduction. In the e\ aluation of chronic anterior instability. a Weht Point view or an apical oblique view, both of which are helpful in the evaluation of anterior glenoid rim defects. and ;I Stryker notch view or an AP \~ew with the arm in internal rotation. to evaluate the posterior humcr-al head for a possible Hill-Sachs det’ctt. mav also provide helpful information. Radiographs allow the sub-classification of anterior dislocLition. Sub-acromial dislocations are the most common. with subglenoid. sub-clavicular and intrathoracic antcrlor dislocations being other variants. MU~U/,YCVIVII~. A closed reduction 01’ an anterior shoulder dislocation should be attempted ;I> \oon a\ the appropriate evaluation has been perform&. After the administration of appropriate analgesic5 anti muscle relaxants, a closed reduction is attempted. Tht least traumatic m&hod of reduction is imperative The Stlmson technique with the patient prone and the arm hanging cover the side of the bed with traction applied. or traction-countertraction maneu\ t‘rs are generally successful and are reasonably atraumatic. 246 CURRENT ORTHOPAEDICS-MINI-SYMPOSIUM: Occasionally, general anesthesia is required for closed reduction, and rarely an open reduction is necessary. Following a successful reduction, X-rays should be obtained to document a satisfactory reduction and rule out any associated fractures. The care after reduction of an initial dislocation is controversial. We would like to know what role post-reduction immobilization and rehabilitation play in limiting the incidence of recurrent instability, which is the most common complication of an acute traumatic anterior dislocation. Unfortunately the literature offers varying opinions regarding the value of immobilization and rehabilitation. In Rowe’s classic study of over 300 anterior dislocations, the redislocation rate in patients under 20 years of age was 945:. This followed immobilization of 3 weeks or less. Hovelius recently compared a group immobilized for 3-4 weeks in a sling and swathe to an early motion group which used a sling only as needed for comfort. He found that immobilization for 3-4 weeks did not reduce the recurrence rate and that age at the time of initial dislocation was the most important factor with regard to prognosis. ‘(’ During his 5-year follow-up, there were two or more redislocations in 55% of patients 12-22 years old, in 37:/i of those 23329, and only 12% of those 30-40 years of age.” Simonet and Cofield,” found that 56% of patients restricted from resuming sports activity for 6 weeks or greater had satisfactory results, compared with only 157; of patients restricted less than 6 weeks. The recurrence rate was 820/, in athletes, compared to 3076 m non-athletes. Yoneda reported that in those treated with 5 weeks of immobilization and subsequent internal rotator strengthening, the redislocation rate was only 17%. I3 In a study at the US Naval Academy, Aronen et alI5 reported only a 257; redislocation rate with a 3-year follow-up in a group treated with muscle strengthening and activity restriction until the rehabilitation goals were met. We presently immobilize the young athlete in a sling for comfort only and then begin early motion and shoulder strengthening, emphasizing rotational strengthening. We also limit the athlete from placing the arm in the provocative position of abduction extension and external rotation for 6-8 weeks following the dislocation. Return to athletics is permitted when the patient achieves a full painless range of motion, normal strength, and has a negative or minimal apprehension sign. There are patients in whom the apprehension sign remains positive. Recurrent anterior instability. Recurrent anterior instability is a very common reason for presentation. As we discussed earlier, recurrent anterior instability needs to be sub-classified in order to adequately discuss its diagnosis and treatment. Recurrent anterior instability may be traumatic or atraumatic. It may be voluntary or involuntary, and it may present as recurrent dislocations, subluxations. or both. History. The patient usually volunteers that ‘my shoulder comes out’. The patient can usually tell if the THE SHOULDER shoulder dislocates, subluxes or does both. The patient is often confused as to the direction of instability so certain questions are important. The position of the arm at the time of the symptomatic instability is extremely important. A patient with instability when the shoulder is abducted, externally rotated and extended, almost certainly has anterior instability. While one with instability with the shoulder in forward flexion, adduction and internal rotation in all likelihood has posterior instability. Complaints of instability while carrying heavy loads, with downward traction applied, are generally related to inferior instability. A history of apprehension is also a very important clue. The apprehensive patient is fearful of putting the arm in a certain position because it ‘may go out’. Patients with recurrent anterior instability are therefore placed into different groups based on their presentation. Recurrent traumatic imoluntary instabilit>l 1. Recurrent dislocations. This group represents those patients with a normally functioning shoulder, until with an inciting event, a dislocation occurs. The dislocation usually requires reduction by another individual, and is generally quite painful. These events may be frequent or infrequent, and may gradually occur with less and less trauma as the shoulder’s stabilizing mechanisms become more incompetent. 2. Recurrent subluxations. The patient with recurrent subluxation who has never had a documented dislocation can present a diagnostic challenge. These patients generally present in one of two ways. Some present with a classical ‘dead arm syndrome’. They may give a history of pain, clicking, and grinding in the shoulder. The ‘dead arm’ feeling has been described in different ways. It can be a ‘sudden sharp paralyzing pain’ (Rowe) or a feeling of heaviness, numbness or weakness associated with the shoulder positioned in abduction, external rotation and extension. The patient may volunteer a history of the shoulder slipping out of place. The second type of presentation in those with recurrent subluxation presents more of a diagnostic challenge. These patients present with a chief complaint of pain in the shoulder. They usually have pain when performing overhead activities suchas throwing. These patients are usually young and have primary anterior instability with secondary tendonitis due to impingement or eccentric overload. Physical examination findings are important in the proper diagnosis of patients in this category. 3. Recurrent dislocation with subluxation. This group represents patients with both recurrent dislocations and subluxations. Due to the frequent episodes of subluxation they are often quite disabled. 4. The ‘apprehension shoulder’ plus 1. 2, or 3. Finally there is a group of patients who although having an underlying instability problem, present with what is best described as an ‘apprehension shoulder’. They _ live a f’earful existence that their shoulder will ‘go out’ if their arm goes into the position of abduction and external rotation. They avoid this position and may become significantly disabled. They often refuse to participate in certain sporting and work related activities. They inevitably develop a limitation ot external rotation. sometimes even with the arm at their side. The physical examination should include a general appreciation of the musculo-skeletal system and then more specifically. the involved and uninvolved shoulders. Features such as an ability to touch the volar forearm with the thumb, hyperextension of the elbows and knees, hyperextension of the fingers to bring them parallel to the dorsal forearm. and an ability to place the palms flat on the floor with the knees extended are important indicators of generalized laxity. These signs are more common in patients with multi-directional and atraumatic instabilit). Instability ways. of the shoulder may be manifest in several I. Apprehension signs or provocative testing suggestive of an underlying instability pattern. 3 Excessive translation of the humeral head within _, the glenoid socket. 3. The obvious presentation of a dislocation or the demonstration on behalf of the patient of an instability pattern. The positive ‘apprehension sign’ is most commonly applied to anterior uni-directional instability of the shoulder. In the sitting position this is performed with the examiner behind the patient stressing the arm in external rotation and abduction. With the arm in this position. controlled levering of the humeral head anteriorly. while palpating directly anteriorly to prevent .I dislocation, will eiicit a feeling of apprehension from the p:ltient (i.e. ‘Crank Test’). This apprehension is manifest by muscle contraction to resist movement, or by an obvious look of apprehension on the patient’s face. or by the patient stating that the maneuver reproduces his functional instability and that they fear the shoulder will ‘come out’ if the stress is continued. Paln may be present, but alone it does not constitute a positive apprehension sign. The ‘apprehension’ maneuver may also be performed with the patient supine (i.e. ‘Fulcrum Test’). The shoulder joint is positioned on the edge of the table. which acts as a fulcrum, with the body providing the counterweight. In this position progressive external rotation, abduction and extension may elicit an ‘apprehensive’ response. _.__-. Trmslution __-__ SHOULDER INSTABILITY -_ ..___ 247 __ of'the gleno-humeral,joint Assessment and grading of the amount of anterior and posterior translation of the humeral head in the glenoid socket is an evolving science. It is often difficult, even with the patient anesthetized, to accurately determine anterior and posterior translation. We use a ‘load and shift’ test which is performed with the patient both sitting and supine. With the examiner sitting to the side and behind the seated patient, the patient’s scapula is fixed with one of the examiner’s hands. The examiner then grazps the humeral head from the lateral side, loading it medially Into the glenoid fossa to insure appropriate reduction and a ‘neutral’ position. The examiner then translates the humeral head posteriorly and then back to the glenoid, this is performed several times until the examiner is sure of the degree of posterior translation. After loading the humeral head into the glenoid, the humeral head is translated anteriorly to determine the anterior translation. The patient’s arm is at his side during this test in the neutral position. The ‘load and shift’ test is then performed with the patient supine. With the patient supine the arm can be placed in different poGtions to assess the integrity of the various component\ of the capsule-labral complex. Inferior translation is determined with the patient seated with his arm at his side. The examiner applies traction to the arm. pulling the humeral head inferiorly. With his other hand the examiner places his thumb and Index finger anterior and posterior to the acromion. pushing the humeral head inferiorly ;I visible ‘sulcus sign’ may he present if there i\ significant inferior translation. It i\ Important to grade the amount of’ translation compare it to the non-involved shoulder. Cir-ade 1 Grade 7 and Translation of the humeral head up the glenoid face to the glenoid rim. Translation of the humeral head over the glenoid rim, with spontaneous reduction upon release of the applied ctress may occur but is still Grade 2. In addition to using the above grading system for anterior. posterior and inferior translation. we also document the centimeters of inferior translation with applied stres\. In addition to grading the translation the examiner should attempt to determine if the translation is symptomatic. If the patient complains of instability. pain or a click with translation in a certain direction. and appreciates that as part of his symptom complex, then the diagnosis is clearer. Relowtion test The ‘relocation test’ described by Jobe and Fowler IS a helpful adjunct in thediagnosisofanterior instability. It is particularly helpful in cases where there is only 248 CURRENT ORTHOPAEDICS-MINI-SYMPOSIUM: anterior subluxation present or when the patient has impingement and rotator cuff tendonitis with underlying anterior instability. In these cases the apprehension sign may be negative, or cause only pain but not apprehension, and translation may be normal. The ‘relocation test’ is performed with the patient, positioned supine as described for the ‘apprehension’ maneuver. The ‘apprehension’maneuver with the arm in abduction and external rotation is performed. The examiner should document any apprehension and pain elicited, and the amount of external rotation achievable. Next the same maneuver is performed but with his other hand the examiner applies a posteriorly directed force to the proximal humerus. This force may ‘relocate’ the humeral head preventing anterior subluxation. This may eliminate apprehension and/or pain and may increase the degree of external rotation achievable. These findings may be consistent with anterior subluxation. We have modified this test by suddenly releasing the posteriorly direct force-the ‘release test’-to see if there is the immediate onset of apprehension and/ or pain. Jobe has also described a modification of his maneuver which we call an ‘augmentation test’. In this case an apprehension maneuver is performed. but an anteriorly directed force is applied to the posterior aspect of the proximal humerus, thus increasing any existing anterior subluxation. This test may be positive for an increase in apprehension and/or pain. Management ofchronic recurrent traumatic involuntary anterior instahilit~ The treatment options of any shoulder instability are acceptance of the disability, rehabilitation, or surgical stabilization. The indications for surgery are based on the patient’s symptoms and disability. The disability is dependent on the frequency of the dislocations, the ease or difficulty of reduction, the age and activity requirement of the patient, and the presence of subluxations and/ or apprehension. The patient with frequent subluxations and apprehension with his arm in abduction/ external rotation is often quite disabled, whereas one who dislocates every 5 years or so, without intervening subluxation and/or apprehension may function quite well without significant disability. If one is not very disabled then we would recommend a non-operative approach. Rotator cuff, trapezius, and serratus anterior strengthening, along with avoidance of the provocative position may be successful. Like many others, however, we have not found rehabilitation to be very successful in young athletic patients with recurrent anterior instability. Surgical options. The main goals of surgery are to stabilize the shoulder and maintain a full, pain-free range of motion. We feel that these goals are best achieved by correction of any pathology-i.e. ‘the essential lesion or lesions’-found at surgery. THE SHOULDER Many different procedures have been described, but many are extra-articular procedures which ignore the existing pathology and distort the normal anatomy. Many times a procedure is successful in preventing recurrent instability at the expense of a significant loss of external rotation, which may rarely lead to the development of osteoarthritis. The different procedures can be divided into: 1. Bony procedures (osteotomies of the glenoid humerus, bone block procedures) 2. Musculo-tendinous operations 3. Capsulo-labral operations 4. Combinations and modifications of the above. or While we do not wish to describe all of the procedures in detail, we feel that in a review article such as this we should comment on some of the more commonly performed procedures. Rockwood in a review of 53 studies. with 3332 cases, found an average recurrence rate of only 37$’ 5 He found that the problem was not the rate of recurrence but often poor function. The recurrence rates were 3.1 “/n for a PuttiPlatt, 4.1:; for a Magnuson Stack, 1.79; for a Bristow and 3.57; for a Bankart respectively.? Putti-Platt. The Putti-Platt has been used for many years, initially independently by Putti and Platt, for recurrent anterior instability. It has undergone many modifications, but in essence, it involves shortening and overlapping of the subscapularis and anterior capsule. While this procedure has generally been reasonably successful in preventing recurrent dislocations, it is almost always accompanied by a significant loss of external rotation. In a long-term review of 132 Putti-Platt procedures, Morrey and Janes, ih found 18 recurrent dislocations for a recurrence rate of 13.6?;. While this recurrence rate is higher than that reported by other series, their’s represented reasonably long-term follow-up. In a functional analysis of Putti-Platt procedures, Regan et al i’ found a 21.8” deficit of external rotation with the shoulder at neutral and a 28.8’ deficit with the shoulder at 90“ of abduction. None of the eight patients who were overhand or throwing athletes returned to their pre-operative level following surgery. Leach et ali” reported a 12-19” loss of external rotation but not functional compromise. While the Putti-Platt procedure may effectively limit anterior instability, we feel that it should not be used as a routine procedure. In addition to limiting external rotation and compromising overhand function, the author has seen several patients who have developed osteoarthritis following an excessively tight Putti-Platt repair.” Magnuson-Stack. In the operation devised by Magnuson and Stack, the anterior capsule and subscapularis tendon are tightened by advancing them laterally on the humerus. As with the Putti-Platt this procedure although reasonably effective in eliminating anterior instability. is often accompanied by an undesirable loss of external rotation. __ Miller et al’” in a review of 29 patients found five post-operative dislocations, a redislocation rate of 17”“. They also found a 25” lack of external rotation and found that only 52”/, returned to their preinjury level of competitive athletics. Karadimos, in the largest single series of Magnuson-Stack procedures ( I54 patients) reported only a ?“,I recurrent rate.:” Regan et al“ found a deficit of 4.7. of external rotation with the shoulder at neutral and a 6.4” deficit with the shoulder at 90” of abduction. They found that three of eight athletes returned to their pre-operative level of throwing and overhand activity. Despite the f-act that the senior author (RJH) had had excellent results with a modified Magnuson-Stack procedure, we rarely perform it anymore. preferring instead to address and repair the pathology. Bristmc,. In 1954 Latarjet described transfer of the coracoid process through the subscapularis tendon as a method of treating anterior instability. Helfet in 1958 described a transplant of the coracoid with the attached conjoined tendon to the anterior surface of the glenoid, through a tranverse rent in the subscapularis muscle. He termed this the Bristow procedure. Mead in 1964 described fixing the bone block with a screw. It has been proposed that the Bristow operation is effective because the coracoid acts as a bone block impeding anterior redislocation, because the cnnjoined tendon acts as a dynamic sling holding the humeral head posteriorly when the arm is abducted and externally rotatecl, and thirdly because it prevents the lower portion of the subscapularis from riding superiorly with abduction, thus reinforcing the anteroinferior capsule.” Many authors have reported excellent result with the Bristow procedure. Hill et al” found only two post-operative dislocations following 83 procedures performed for anterior dislocation, but found that five of 24 patients operated on for anterior subluxations continued to have subluxationspost-operatively. Their redislocation rate was similar to that reported by Allman who found no redislocations in 50 cases, Collins and Wilde who also had no redislocations in 50 cases, and Sweeney et al who had a 3”” redislocation rate in 97 cases. Hovelius et al in a review of I I3 cases, found a redislocation rate of 6”, and a resubluxation rate of 7”,,. Torg et al reported a post-operative instability rate of X.5”,, in a series of 207 modified Bristow procedures.” Unfortunately, most authors have reported significant losses of external rotation and diminished athletic function following the procedure. Hill et al” found a mean loss of external rotation of 12.6 and found that only six of 41 patients could throw in the same manner as before injury. Regan et al” found a 12.2” deficit of external rotation with the shoulder at neutral and an 11.6” deficit with the shoulder at 90 of abduction. In their series only three of nine throwers returned to their prior performance level. Torg et a1 in a large series found that only 16”” ._~ --- SHOULDER INSTABILITY -_-- ‘49 of athletes whose dominant arm had been operated on returned to their pre-injury level of throwing.” We do not recommend routine use of the Bristow procedure due to the potential problems with the screw,’ ’ potential injury to the musculocutaneous nerve, marked distortion of the normal anatomy. and loss of external rotation. However, it may have a role Mhen used in a situation in which there has been a significant bony loss of the anterior gelnoid rim. Budart prowdurr. The Bankart procedure is a capsular repair first performed by Perthes in 1906. It was popularized by Bankart’s article in 1939 describing the repair of the anterior capsule to the hone of the anterior glenoid through drill holes with the use of a suture. A Bankart repair or a modification of it is currently the ‘gold standard’to which other procedures should be compared. The main advantage of the Bankart is that it directly addresses the pathology perpetuating the instability, as a Bankart lesion is the most common pathology associated with traumatic anterior instability. The procedure :~lso allows the surgeon to modify the case intra-operatIvei? and pert’orm an anterior capsulorrhapy or a capsular shift if only capsular redundancy is found. The Bsnkart procedure cim also be performed without causing a significant loss of external rotation. Rowe has been a major proponent of the Bankart or modified Bankart repair. Rowe and Zarinsi reported ;I series of 50 shoulders with anterior subluxation. A Bankart procedure was performed in the 32 shoulders In which a Bankart lesion c\as found, and a modified Bankart repalr (capsulorrhapy) was performed in the remaining IX p;itients who had capsular redundancy Good or excellent result were obtained in 94O, oi‘ the caseh. HoLelius et al found a 200 redislocation rate Clfter the Bankart procedure compared with ;i 19”,, redi&~cation rate after the Putti-Platt. Several authors have reported good function and only small deficits of external rotation following a Bankart procedure. in Rowe’s series there were ?? dominant shoulders, with 21 of these (64”“) able to return to forceful throwing and participate In sports and work. Author’.~ prrfewti approach. Our philosophy has now evolved such that we utilize an approach that allows dealing with any pathology present at the time of surgery. This is our current method despite consistent result\ in the past with a modified Magnuson-Stack procedure. We utilize two varieties of soft tissue repair based upon ;tccess to the shoulder joint. I. Our first approach is almost identical to that recently described by Thomas and Matsen. ‘1 Through a standard delto-pectoral approach we make an incision through the subscapularis tendon and capsule I cm medial to the biceps tendon in a vertical fashion. The joint is then explored both visually and by direct palpation to assess the pathology. If there is a detached labrum it 1s re-attached through drill holes to the bony glenoiti rim. If the capsule is stripped with a 250 CURRENT ORTHOPAEDICS-MINI-SYMPOSIUM: degenerative labrum the capsule is sutured down to the glenoid rim making sure that tethering the overlying subscapularis with sutures is avoided. If anterior capsular redundancy is present, the capsule, and sometimes subscapularis are shortened and tensioned, ensuring 20” of external rotation is obtained at the completion of the procedure. 2. The second technique is more technically demanding but allows for more direct capsular plication. This approach involves incising through the subscapularis tendon in a vertical fashion separating it from the underlying capsule. A ‘T’ shaped incision based laterally is made through the capsule with the horizontal arm of the ‘T’ extending medially to the glenoid. The pathology is then addressed accordingly, either repair of the labrum and/or capsule to the bony glenoid as above, or plicating the two flaps of capsule in a cruciate fashion (i.e. an anterior capsular repair) is performed. The advantage of this approach is that the subscapularis is not shortened. We have uncommonly used a subscapularis splitting approach, as popularized by Jobe, in throwing athletes. This may allow earlier rehabilitation and less restriction of external rotation, as yet unproven. Controversies related to anterior instability and impingement As mentioned above, young athletes with anterior subluxation often present with pain and symptoms related to impingement and rotator cuff tendonitis. The patient with impingement and instability is generally a young overhand or throwing athlete. The primary pathology is either congenital capsular laxity or acquired capsular laxity from the frequent stresses incurred during the throwing motion. The capsular laxity allows increased humeral translation, resulting in fatigue and eccentric injury to the rotator cuff and parascapular muscles. Muscle dysfunction and fatigue lead to loss of the normal depressor effect of the rotator cuff, allowing the humeral head to migrate proximally and anteriorly, where impingement on the overlying coraco-acromial arch is possible. Physical findings include positive impingement signs, but signs of subluxation are often subtle. The apprehension sign may be positive, but often elicits only pain. The relocation test is often helpful in this case, usually relieving the pain brought on by the apprehension maneuver. Often an exam under anesthesia along with arthroscopy of the shoulder are helpful in making the diagnosis. The initial treatment is a conservative program emphasizing rotator cuff and parascapular muscle strengthening. In most, this program is successful, but if surgery becomes necessary it may be prudent to address the instability. An anterior cruciate capsulorrhaphy or a Bankart repair in the presence of a Bankart lesion is usually our recommended approach. Subacromial decompression may be unsuccessful if performed without addressing the instability, yet THE SHOULDER sometimes it is a first step to try, as it is a lesser procedure and may eliminate symptoms. Arthoscopy. Diagnostic arthroscopy particularly as an aid in the diagnosis of subtle instability, has a role in the management of anterior instability. Arthroscopy allows inspection of the anterior glenoid rim, capsularlabral complex, the rotator cuff, and the posterior humeral head. A Bankart lesion, labral damage, or a Hill-Sachs lesion suggest anterior instability. In those with associated rotator cuff tendonitis and impingement one may find a partial thickness, joint surface cuff tear suggestive of eccentric injury, or subacromial changes suggesting impingement. The role of arthroscopy in anterior reconstruction is still undefined. Johnson, Caspari, Morgan and Matthews have reported variable results from arthroscopic capsular-labral repair. Morgan reported on 25 patients with recurrent anterior dislocations treated with arthroscopic suturing of a Bankart lesion. At 17 months follow-up, there were no instances of recurrent instability.” Matthews et alZb reported on 25 patients with recurrent anterior instability treated with arthrostopic staple capsulorrhaphy. Five patients were reoperated on for pain/or recurrent instability. Johnson has also reported about a 20% failure rate following arthroscopic staple capsulorrhaphy. Caspari has reported improved results using an arthroscopic technique utilizing sutures to repair the capsular-labral complex. Presently we feel that open procedures remain the treatment of choice. However, with better instrumentation, such as biodegradable screws and staples presently being evaluated, further experience, longer follow-up and careful comparison with traditional open techniques, arthroscopic stabilization may ultimately become the treatment of choice in some cases. Recurrent atraumatic anterior inooluntary instabilit) The basic assessment and management of atraumatic instability differs little from traumatic instability. This group obviously presents with a different history. The initial dislocation or subluxation occurs without a significant traumatic event, often occurring during the acts of throwing or swimming. The important difference from traumatic instability is that the pathology or ‘essential’ lesion is usually not a Bankart lesion. These patients usually have capsular laxity. either congenital or acquired, and only occasionally have a Bankart lesion. There is often a component of multi-directional instability in this group. The treatment differs in that we recommend a longer trial of conservative management, emphasizing rotator cuff and parascapular muscle strengthening. If conservative treatment fails then a specific capsulorrhaphy, addressing the laxity is indicated. In general we prefer an anterior cruciate type capsulorrhaphy, sometimes in conjunction with an inferior capsular shift. The failure rate of extra-articular procedures SHOULDER such as a Bristow, Putti-Platt. of concern in this group. or Magnuson-Stack is Postrrior dislocation. Traumatic dislocations are rare, accounting for only about 2”” of all traumatic dislocations. The diagnosis is often missed initially. In a review of 41 locked posterior dislocations by the senior author,‘the correct diagnosis was made between I and 6 weeks after injury in 13 cases, between 6 weeks and 6 months in 12 cases, and after 6 months in I6 cases. The mechanisms of injury included motor cehicle accidents (16 cases), seizures (11 cases). electro-shock treatments (eight cases), and alcoholrelated injuries (six cases). Physical examination revealed a loss of external rotation, with an average internal rotation deformity of 40”. There was also a loss of supination. The axillary X-ray was diagnostic in all cases. but had not been obtained initially in any case. A fracture of the lesser tuberosity seen on an AP radiograph is also an indication that there may be a posterior dislocation. If a traumatic posterior dislocation in the absence of an impression defect is diagnosed acutely. management consists of a closed reduction and immobilization in a spica cast with the shoulder externally rotated and extended. The treatment of a locked posterior dislocation depends on the duration of the dislocation and the size of the humeral head defect. The guidelines are as follows : I. Closed reduction ~-Duration less than 6 weeks and Defect less than 20”, A. 7 Lesser Tuberosity Transfer-(Modified McLaughlin Procedure) ~~Duration less than 1 year and -Defect 20 50”. of humeral head 3. Hemlarthroplasty Duration greater than 1 year and/or Defect greater than 50”,, If a hemiarthroplasty is performed it should be placed in neutral version rather than retroversion to decrease the incidence of postoperative posterior instability. Rtwrrmt po.stcvYrw .suh/u.wtion. Posterior instability is usually subluxation rather than dislocation and seldom requires reduction. Ocassionally there is the history of a traum..itic injury. but more commonly posterior subluxation results from overuse. The patient often complains 01‘ pain and instability with his arm in forward f&ion. adduction and internal rotation, Classitication Includes habitual, voluntary and involuntary variants. Physical findings include increased posterior translation. and rarelv a positive posterior apprehension sign performed with the arm in forward flexion, adduction, and internal rotation. The patient is often able to demonstrilte the subluxation with provocative INSTABILITY 251 positioning and/or muscle contraction. A small percentage of these patients are psychiatrically disturbed. Treatment consists of prolonged non-operative management. Rotator cuff strengthening. stressing the external rotators and parascapular muscles is emphasized. Posterior surgical reconstructions are far less successful than anterior procedures. In a review by the senior author,‘X the recurrence rate was 50”” in 26 patients operated on for recurrent posterior subluxation. Our preferred posterior reconstruction is a softtissue procedure including posterior capsular and infraspinatus shortening. We use a spica cast postoperatively and proceed cautiously with rehabilitation. With our recent surgical changes. results are much improved. Mlriti-tlirc~c,tional instabilit?, Multi-directional instability (MDI) was introduced as a concept by Neer in 1980.” Since that time it has been recognized as a much more common problem then previously realized. The hallmark of multidirectional instability if symptomatic inferior instability In association with anterior and’or posterior instability. Neer has taught us that the etiological factors contributing to MD1 include various combinations of: 1. Repetitive overuse ._. 3 Inherent ligamentous/capsular 3. Major traumatic injuries laxity MD1 is seen in athletes as well as sedentary individuals. Proper detection depends on suspecting the possibility of MDI. The patient often complains of the shoulder ‘slipping down’ while carrying heavy loads. In addition, the patient may complain of anterior and/ or posterior instability with the arm in the respective pro\ ocative position. Many patients with MD1 present with a chief complaint of pain. Often the patient has problems with the opposite shoulder or instability of other joints. The hallmark of MD1 is a positive sulcus sign as described above. In addition there is increased anterior and posterior translation. Signs of generalized ligamentous laxity as described above are frequently present. The treatment again consists of prolonged internal and external rotator strengthening. These patients often have scapular dysfunction and winging. and require parascapular muscle strengthening. If non-operative treatment fails then surgery should be considered. Standard operations for uni-directional anterior or posterior dislocations may fail to correct MD1 because the pathology is not corrected. The main pathology is increased joint volume due to an enlarged inferior axillary capsular pouch. The standard procedure may not correct inferior instability and may displace the head to the opposite side leading to arthritis. Neer”’ introduced the inferior capsular shift 252 CURRENT ORTHOPAEDICS-MINI-SYMPOSIUM: for MD1 and this is the procedure that we perform. This is generally performed from an anterior approach, but in some cases of posterior-inferior instability, it is performed through a posterior approach in conjunction with an infraspinatus shortening. Summary The proper diagnosis and classification of shoulder instability allows the physician to recommend the appropriate treatment. Rehabilitation is the preferred treatment for posterior subluxation and MDI. Recurrent anterior instability generally requires surgery for optimal function. Surgery can be very successful in preventing instability and allowing a normal range of motion if the pathology causing the instability is corrected. References 1990; W 1. Rockwood C, Matsen F. The Shoulder. Philadephia: B Saunders Company 2. Rowe C. The Shoulder. New York: 1988; Churchill Livingstone following an excessively tight 3. Hawkins R J. Osteoarthritis Putti-Platt repair. OrthoTrans 1988; 12(3): 728 4. Rowe C, Pate1 D, Southmayd W. The Bankart procedure. J Bone JointSurg 1978;6OA(l): 116 5. Rowe C. Zarins B. Recurrent transient subluxation of the shoulder. J Bone Joint Surg 1981; 63A(6): 863872 6. Rowe C, Zarins B. Ciullo J. Recurrent anterior dislocation of the shoulder after surgical repair. Apparent cause of failure and treatment. J Bone Joint Surg 1984; 66A: 159 I. Rowe C, Pierce D, Clark J. Voluntary dislocation of the shoulder. J Bone Joint Surg 1973; 55A(3): 445460 8. Hovehus L. Incidence of shoulder dislocation in Sweden. Clin Orthop 1982; 116: 127 9. Rowe C. Prognosis in dislocations of the shoulder. 1956; 38A(5): 957-977 10. Hovelius L, Eriksson K, Fredin H. Hagberg G, Hussenius A, Lind B, Thorling J, Weckstrom J. Recurrences after initial dislocation of the shoulder. J Bone Joint Surg 1983; 65A(3): 343.-349 11. Hovelius L. Anterior Dislocation of the Shoulder in Teenagers and Young Adults: Five-year prognosis. J Bone Joint Surg 1987; 69A: 393-399 THE SHOULDER 12 Simonet W T, Cofield R H. Prognosis in anterior shoulder dislocation. Am J Sports Med 1984; 12: 19 13 Yoneda B, Welsh R P, Macintosh D L. Conservative treatment of shoulder dislocation. J Bone Joint Surg 1982: 64B r254 14 Aronen J G. Regan K. Decreasing the incidence of recurrence of first time anterior shoulder dislocation with rehabilitation. Am J Sports Med 1984; 12: 283-291 I5 Rockwood C, Green D. Factures in Adults. Second Edition. Philadelphia: 1984; J B Lippincott Company 16 Morrey B, Janes J. Recurrent anterior dislocation of the shoulder. J Bone Joint Surg 1976; 58A(2): 252-256 S, Hawkins R, Fowler P. 17. Regan W, Webster-Bogaert Comparative functional analysis of the Bristow, MagnusonStack, and Putti-Platt procedures for recurrent dislocation of the shoulder. Am J Sports Med 1989; 17(I): 42248 18. Leach R E, Corbett M, Schepsis A et al. Results of a modified Putti-Platt operation for recurrent shoulder dislocations and subluxations. Clin Orthop 1982; 164: 20-25 19. Miller L, Donahue J, Good R. Staerk A. The Magnuson-Stack Procedure for Treatment of Recurrent Glenohumeral Dislocations. Am J Sports Medicine 1984; 12(2): 1333137 20. Karadimas J, Rentis G, Varouchas G. Repair of recurrent anterior dislocation of the shoulder using transfer of the subscapularis tendon. J Bone Joint Surg 1976: 58A: 256 261 21. Hill J, Lombard0 J. Kerlan Jobe F. Carter V. Shields C, Collins H. Yocum L. The modified Bristow-Helfet procedure for recurrent anterior shoulder subluxations and dislocations. Am J Sports Medicine 1981; 9(5): 2833287 22. Torg J S, Balduini F C, Bonci C et al. A modified BristowHelfet-May procedure for recurrent dislocation and subluxation of the shoulder: Report of Two Hundred and Twelve Cases. J Bone Joint Surg 1987; 69A: 904-913 about the glenohumeral joint 23. Zuckerman J. Complications related to the use of screws and staples. J Bone Jomt Surg 1984; 66A(2): 175-180 24. Thomas S C. Matsen F A III. An approach to the repair of avulsion of the glenohumeral ligaments in the management of traumatic anterior glenohumeral instability. J Bone Joint Surg 1989: 71A: 506 Bankart suture repair: 25. Morgan C. Bodenstab A. Arthroscopic technique and early results. J Arthroscopic Related Surg 1987; 3(2): 111~122 26. Matthews L, Vetter W. Oweida S, Spearman J, Helfet D. Arthroscopic staple capsulorrhaphy for recurrent anterior shoulder instability. J Arthroscopic and Related Surg 1988; 4(2): 106~11 I 27. Hawkins R J. Neer C. Pianta R et al. Locked posterior dislocation of the shoulder. J Bone Joint Surg 1987; 69A : 9 -18 28. Hawkins R J, Koppert G. Johnston G. Recurrent posterior instability (subluxation) of the shoulder. J Bone Joint Surg 1984; 66A(2): 1699174 29. Neer C, Foster C R. Inferior capsular shift for involuntary inferior and multidirectional instability of the Shoulder. A Preliminary Report. J Bone Joint Surg 1980: 62A: 897,908