Uploaded by
common.user17333
Gitelman Syndrome Case Report: Periodic Paralysis & Anemia
advertisement

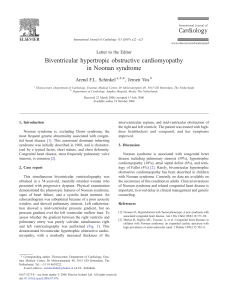
GITELMAN SYNDROME WITH PERIODIC PARALYSIS AND ANEMIA Case Report M Saiful Rahman-Leonita Anniwati The 8th SURAMADE Malang, July 9th-14th 2018 Department of Clinical Pathology Faculty of Medicine Airlangga University, Surabaya Dr. Soetomo Hospital Indonesia , Preeliminary Gitelman syndrome is an autosomal recessive disorder in the kidney that is marked by clinical symptoms of : • Normal or low blood pressure • Decreased levels of potassium and magnesium serum • Increase in blood PH levels. Disorder is caused by a mutation of the SLC12A3 gene located on chromosome 16q13 encoding thiazide-sensitive sodium-chloride cotransporter (NCC, NCCT, or TSC) 2 The prevalence of Gitelman syndrome is estimated to be 1 : 40.000 births The diagnosis of Gitelman syndrome is based on clinical symptoms along with laboratory tests that include : 1. Hypokalemia 2. Hypomagnesemia 3. Metabolic alkalosis 4. Hypocalciuria. 3 Case MC HI HPI AR 13 Y.O Body weakness 3 days before hospital admission with acute paralysis, pain and weakness in the extremities of a limb one day before admission. fever (+) convulsion (-) vomiting (-) diarrhea (-). Trauma (-), 4 Physical Examination PE : weak, alert BP : 118/68 mmHg PR : 95 x/minute RR : 26 x/minute t : 36.7oC H/N : A-/ J-/ C-/ D- Chest : H: S1S2 single, gallop (-), murmur (-) Abd L: ves/ves Rh -/- Wh -/- : flat, bowel sound (+) N L/S : not palpable 5 Ext : warm, edema (-) Neurologic examination showed : • Physiological reflex of + 2 / + 2 in the upper extremity and + 1 / + 1 in the lower extremity • The pathologic reflex Chaddok reflex(-), Babinsky reflex (-). Sign of bleeding : (-) 6 Clinical Chemistry BUN (mg/dL) November (admission) I 14.3 II III IV Reffrence Range 8.0 10 - 20 0.6 3.2 138 1.1 93 7.0 0.8 294 179 1096 0.6 – 1.3 3.4 – 5.0 136 -145 3.5 – 5.1 98 - 107 8.5 – 10.1 1.8 – 2.4 < 50 < 50 10 - 20 150-990 Phosphatase Urine (mg/24h) Creatinine Urine (mg/24h) 500 300-1000 1304 600-2000 Calcium Urine(mg/24h) 120 50-400 Potassium Urine(mg/24h) 25.6 35-80 Natrium Urine(mg/24h) 120 30-300 Chlorida Urine(mg/24h) 160 85-170 SCr (mg/dL) Albumin (g/dL) Na (mmol/L) K (mmol/L) Cl (mmol/L) Calcium (mg/dL) Magnesium AST (U/L) ALT (U/L) Phosphatase (mg/dL) Uric acid Urine (mg/24h) 1.15 132 1.4 94 134 1.1 86 7.1 0.5 1787 419 Serum Iron (mg/dL ) TIBC ( mg/dL 47 229 7 131 1.5 91 6.7 0.5 35-150 250-450 Clinical Chemistry November (admission) I II III IV Reffrence Range Na (mmol/L) 132 134 138 131 136 -145 K (mmol/L) 1.4 1.1 1.1 1.5 3.5 – 5.1 Cl (mmol/L) 94 86 93 91 98 - 107 Calcium (mg/dL) 7.1 7.0 6.7 8.5 – 10.1 Magnesium 0.5 0.8 0.5 1.8 – 2.4 8 Blood Gas Analysis Parameters I pH 7,47 pCO2 (mmHg) 39 pO2 89 (mmHg) HCO3 (mmol/L) 28,4 TC02 (mmol/ L) 29,6 BE 4,7 SO2 (%) 83 AaDO2 114 Temp 36,8 9 Metabolic Alkalosis I II III Hb (g/dL) 10.7 9.8 9.2 RBC (X 106/ɥL) 5.1 4.33 4.26 Hct (%) 40.4 35.7 29.7 MCV (fL) 68 82.3 69.7 MCH (pg) 21.5 26.8 21.6 MCHC (g/dL) 31.6 32.5 31.0 RDW (%) 13.6 13.4 16.9 WBC (X 103/ɥL) 17.59 16.87 14.47 Neutrophil (%) 88.8 83.4 80.5 Lymph(%) 6.4 8.9 11.2 Mono(%) 3.9 6.3 5.7 Eo % 0.2 0,2 0,25 Plt x 103/µL 312 302 297 Hematology 10 X- Ray Thorax Photo Normal Plain Abdominal Photo Normal 11 ECG with Prolongation QT wave 12 Discussion Four possible mechanisms can cause hypokalemia: 1. Inadequate potassium intake (ie anorexia nervosa, long-term hunger) 2. Extracellular to intracellular shift of potassium 3. Non-renal loss (ie sweating, vomiting and diarrhea) 4. Excess renal potassium loss Bartter or Gitelman syndromes are a congenital aberration of the renal tubules that provide an image of hypokalemia, metabolic alkalosis and may be accompanied by other clinical and Laboratory abnormalities 13 In this disorder occurs hypokalemia due to renal potassium wasting and normal blood pressure Bartter's syndrome : 1. Antenatal Bartter syndrome 2. Bartter classic syndrome 3. Variant of Bartter syndrome is Gitelman syndrome 14 Tabel 6. Differences in Bartter type 3 syndrome and Gitelman syndrome(12) Gitelman syndrome Hypocalciuria, hypermagnesiuria Hypomagnesemia 15 Conclusion Due to severe hypokalemia, hypomagnesemia, metabolic alkalosis and periodic paralysis this patient was diagnosed as Gitelman syndrome. The diagnosis should be confirmed by molecular DNA diagnostic studies to establish mutations of the gene encoding the thiazide-sensitive Na-Clcotransporter 16 17