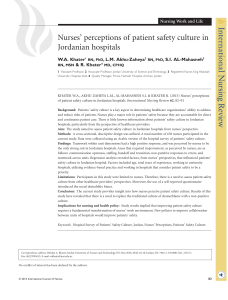
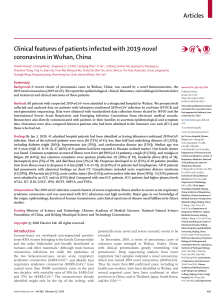
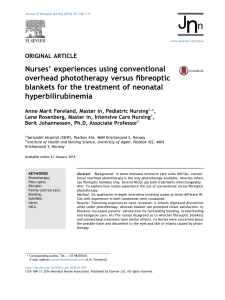
Pulmonary Critical Care I CARE NURSES’ PERCEPTIONS OF ROUTINE DYSPNEA ASSESSMENT NTENSIVE C E 1.0 Hour This article has been designated for CE contact hour(s). See more CE information at the end of this article. ©2020 American Association of Critical-Care Nurses doi:https://doi.org/10.4037/ajcc2020711 132 Background Dyspnea (breathing discomfort) is commonly experienced by critically ill patients and at this time is not routinely assessed and documented. Intensive care unit nurses at the study institution recently instituted routine assessment and documentation of dyspnea in all patients able to report using a numeric scale ranging from 0 to 10. Objective To assess nurses’ perceptions of the utility of routine dyspnea measurement, patients’ comprehension of assessment questions, and the impact on nursing practice and to gather nurses’ suggestions for improvement. Methods Data were obtained from interviews with intensive care unit nurses in small focus groups and an anonymous online survey randomly distributed to nurses representing all intensive care units. Results Intensive care unit nurses affirmed the importance of routine dyspnea assessment and documentation. Before implementing the measurement tool, nurses often assessed for breathing discomfort in patients by using observed signs. Most nurses agreed that routine assessment can be used to predict patients’ outcomes and improve patient-centered care. Nurses found the assessment tool easy to use and reported that it did not interfere with workflow. Nurses felt that patients were able to provide meaningful ratings of dyspnea, similar to ratings of pain, and often used patients’ ratings in conjunction with observed physical signs to optimize patient care. Conclusion Our study shows that nurses understand the importance of routine dyspnea assessment and that the addition of a simple patient report scale can improve care delivery and does not add to the burden of workflow. (American Journal of Critical Care. 2020;29:132-139) AJCC AMERICAN JOURNAL OF CRITICAL CARE, March 2020, Volume 29, No. 2 www.ajcconline.org Downloaded from http://aacnjournals.org/ajcconline/article-pdf/29/2/132/125370/132.pdf by Agus wahyudi on 22 August 2020 By Kathy M. Baker, MSN, RN, Natalia Sullivan Vragovic, MSN, RN, and Robert B. Banzett, PhD P atients receiving mechanical ventilation in intensive care units (ICUs) have described the dyspnea experience thus: “I often thought about death while I was attacked by dyspnea”; “I wondered what’s going on with my breathing, I asked myself ‘will I die here?’”1 Despite evidence that dyspnea causes suffering2,3 and is a predictor of adverse patient outcomes,4,5 little information regarding routine measurement and documentation of dyspnea in the ICU has been published. About the Authors Kathy M. Baker is a clinical nurse specialist and Natalia Sullivan Vragovic is a nurse practitioner in the bone marrow transplant unit, Beth Israel Deaconess Medical Center, Boston, Massachusetts. Robert B. Banzett is an associate professor, Department of Medicine, Division of Pulmonary, Critical Care, and Sleep Medicine, Beth Israel Deaconess Medical Center and Harvard Medical School, Boston, Massachusetts. Corresponding author: Kathy M. Baker, 330 Brookline Avenue (Reisman 1113), Boston, MA 02215 (email: [email protected]). www.ajcconline.org current standards require that organizations establish policies regarding pain assessment and treatment and conduct educational efforts to ensure compliance,18 so clinicians in health care systems worldwide routinely assess and document patients’ pain ratings. Although less common than pain, dyspnea is prevalent in ICU patients and can be more distressing.8,19 In 2013, nurses at our institution began routinely measuring and documenting dyspnea in all medicalsurgical patients using a numeric scale ranging from 0 to 10, with 10 indicating unbearable dyspnea. In 2015, this practice was extended to all ICU patients, and nurses were asked to include dyspnea in routine patient assessments every 4 hours. (Data entry in our electronic documentation system is not mandatory.) We conducted focus sessions and an anonymous online survey to obtain nurses’ feedback regarding routine assessment. Patients on medicalsurgical units who report dyspnea are more likely to suffer serious adverse events in hospital. Methods The study design included a 2-part data collection method with qualitative (focus group interviews) and quantitative (random anonymous survey) components. These studies were approved by the medical center’s institutional review board. Focus Groups In August 2016, we invited ICU nurses to participate in focus groups designed to assess nurses’ perceptions of the utility of routine dyspnea assessment, ease of use, patients’ comprehension of questions, and impact on practice and to collect suggestions for improvement. The location, date, and time of the sessions were arranged with local nursing leaders and invitations were sent to nurses via email 1 week before each session, with a reminder sent the day before the session. Inclusion in the sessions was limited to nurses on duty the day interviews were held, and written consent was obtained. Sessions AJCC AMERICAN JOURNAL OF CRITICAL CARE, March 2020, Volume 29, No. 2 133 Downloaded from http://aacnjournals.org/ajcconline/article-pdf/29/2/132/125370/132.pdf by Agus wahyudi on 22 August 2020 Recent studies show the harmful impact and high prevalence of dyspnea in ICU patients. In one recent study of 30 ICU patients receiving mechanical ventilation, 100% reported breathing discomfort (median score, 4 on a scale of 0 to 10).6 In another study, 47% of 96 patients receiving mechanical ventilation reported dyspnea (median score, 5 on a scale of 0 to 10).7 Dyspnea was reported to be the most distressing of 10 symptoms in a survey of 171 ICU patients.8 Dyspnea in ICU patients is associated with indicators of posttraumatic stress disorder and correlates with duration of mechanical ventilation.3,9-11 Dyspnea is an independent predictor of morbidity and mortality in specific patient populations and is not limited to diseases of pulmonary origin. Dyspnea is more closely associated with cardiac mortality than is angina12,13 and is a more reliable predictor of mortality in patients with esophageal and gastric cancers than are symptoms such as pain, nausea, loss of appetite, and fatigue.14,15 Patients on medicalsurgical units experiencing any dyspnea on admission have greater than a 3-fold odds of death in the hospital.16 Assessing and documenting dyspnea are the first steps in managing this distressing symptom. The American Thoracic Society defines dyspnea as a “subjective experience of breathing discomfort that consists of qualitatively distinct sensations that vary in intensity.”17 This statement emphasizes that dyspnea can be perceived, and thus reported, only by the person experiencing it. Clinicians, including critical care nurses, respiratory therapists, and physicians, can decrease suffering and improve quality of care by asking for dyspnea ratings from all patients who are able to respond. The Joint Commission’s Number of respondents (of 37) 40 30 20 10 0 Important or very important Moderately important to use uniform tool to track every shift for patient-centered care for predicting outcome Figure 1 Nurses’ opinions of the importance of dyspnea assessment. Results Effect on workflow Very positive Positive No effect Negative Very negative 0 10 20 30 Number of respondents (of 37) Importance of Dyspnea Assessment Thirty-seven of 48 surveys were completed (77% response rate). Nurses reported that assessing dyspnea with a uniform tool and tracking dyspnea at every shift are important. They also stated that routine measurement can be useful in predicting patients’ outcomes and can lead to improved patient-centered care (Figure 1). Comments from the survey and focus sessions enhanced the survey finding that nurses believe routine assessment is important: • “I have always completed the dyspnea assess- Figure 2 Nurses’ opinions of the effect of routine assessment on workflow. were held during nurses’ nonpaid lunch breaks in locations near the 8 ICUs. Participation was voluntary, and nurses were allowed to enter and exit throughout the session as necessary. The purposes of the focus groups were to help us tailor the online survey to ICU nurses and to provide verbatim comments to illustrate the survey results. We held two 30-minute focus sessions. Facilitators took field notes and recorded sessions to document discussion accurately. Participants were informed that sessions were recorded and that all identifying information would be omitted when the recordings were transcribed. A staff nurse (N.S.V.) and a clinical nurse specialist (K.M.B.) led the focus sessions. An interview guide was provided to participants to facilitate conversation and ensure that all discussion points were addressed. Seven and 10 nurses representing 6 of the ICUs attended the first and second session, respectively. 134 ment when I assess respiratory distress.” • “Dyspnea assessment was already part of my patient assessment if the patient was able to report their level of respiratory distress.” • “Allows for patient to explain in their own words how they are feeling.” Implementation of Dyspnea Assessment Most nurses (92%) found the assessment tool easy or very easy to administer. Most (68%) noted the addition of dyspnea assessment did not interfere with workflow, and some (32%) said it improved workflow (Figure 2). Comments from the 8% of nurses who found the tool “difficult” to administer included the following: • “There are too many options for the different levels of distress . . . mild, moderate, and severe would suffice.” • “Our patients often cannot rate/score their dyspnea. They don’t understand the scale.” AJCC AMERICAN JOURNAL OF CRITICAL CARE, March 2020, Volume 29, No. 2 www.ajcconline.org Downloaded from http://aacnjournals.org/ajcconline/article-pdf/29/2/132/125370/132.pdf by Agus wahyudi on 22 August 2020 Important Important Important Important Of little or no importance Survey On the basis of experience and information obtained from the focus interviews, we made adjustments to a survey we had previously administered to medical-surgical nurses at our institution19 to better suit the survey to ICU nurses. All of the survey questions and responses are shown in the Supplement (available online only at www.ajcconline.org). In September 2016, the modified survey was distributed via a Web-based software platform (REDCap, hosted at Harvard Catalyst–Beth Israel Deaconess Medical Center) to 48 registered nurses (14% of the ICU nursing staff) selected randomly from each of the ICUs. Nurses were given 4 weeks to complete the survey. Study researchers and local unit leaders sent reminders via email. The survey allowed participants to add comments; some of the more illustrative are included in the Results. Patient is unresponsive the scale simpler . . . normal, worse than normal, worse than it’s ever been before.” • “I typically ask if they are having difficulty breathing or feeling short of breath. If the answer is no, I presume that the number rating is 0/10 as I would presume with the pain scale. . . .” • “I document ‘0’ if the patient responds no if their diagnosis and my assessment support this. [I] ask more questions or rephrase . . . if objective findings suggest otherwise.” • “If the patient does not appear to be in any distress, oxygen saturations are fine on room air, etc, and they report no, I would document a ‘0.’ If their breathing is off baseline, I will investigate further.” Nurses in focus sessions and the survey recalled patients who responded no to the initial question but then gave a nonzero rating. Nurses felt that the initial response of no was often because patients with chronic disorders become accustomed to living with breathing discomfort: • “I have noticed that patients often give themselves a 1-3 rating even when they answer no.” • “A patient with COPD [chronic obstructive pulmonary disease] may say no, but their baseline dyspnea score could be 4, so it is important to obtain the baseline report.” • “Every patient has a different baseline level . . . such as with COPD, asthma patients. It is important to ask the number as their baseline may be 3.” www.ajcconline.org Patient seems more uncomfortable than self-report Patient seems less uncomfortable than self-report 0 5 10 Number of respondents (of 22 total) Figure 3 Reasons nurses use patients’ physical signs rather than patients’ self-reports of dyspnea. Patient’s Report Versus Observed Signs to Assess Dyspnea Dyspnea training for nurses in our hospital includes the concept that dyspnea, like pain, is defined as the patient’s experience, so the patient’s report is the best indicator of severity. However, ICU nurses reported that they often supplement or even supplant patients’ reports with their own estimates from observed signs. Nurses used physical signs to modify patients’ reports most often because the patient was unresponsive or was unable to use the number scale for some other reason. Comments included the following: • “I don’t complete the dyspnea score if the patient cannot give the report.” Downloaded from http://aacnjournals.org/ajcconline/article-pdf/29/2/132/125370/132.pdf by Agus wahyudi on 22 August 2020 Practicalities of Assessment Most nurses reported using more than 1 phrase to explain to the patient what they were supposed to rate. Many (65%) included the phrase “breathing discomfort,” as contained in the American Thoracic Society’s definition of dyspnea. Other phrases commonly used were “difficulty breathing/trouble breathing” (92%), “short of breath” (73%), and “can’t catch your breath” (57%). Most nurses (76%) reported first asking a yes/ no question (eg, “Are you having any breathing difficulty?”) when assessing for dyspnea. For patients who responded no, 42% of nurses said they recorded a score of 0 without asking the patient to provide a number rating. The following comments explain this process: Patient is unable to use scale Reason • “Make • “Often patients are intubated, confused, deliri- ous, or have dementia and cannot answer.” Nurses reported using physical signs rather than patients’ reports twice as often for patients who seemed more uncomfortable than they claimed as for patients who seemed less uncomfortable than they claimed (Figure 3). Nurses reported assessing respiratory distress with the following physical signs listed in the survey (in descending order of frequency of selection): accessory muscle use, tachypnea, difficulty speaking, restless movements, heart rate, nasal flaring, ventilator dyssynchrony, and fearful facial expression. The online survey confirmed that ICU nurses often used some combination of patient’s report and observed signs to obtain a rating for dyspnea; 15 of 36 respondents said they always use a combination. Six nurses report they always used the patient’s report alone, and only 3 nurses said they always used physical signs alone. Nurses in the focus groups and in the survey suggested that a solution to this conflict might be to provide a separate scale allowing nurses to report their respiratory distress estimates according to observed signs. Comments regarding the use of observed physical signs rather than the patient’s report included the following: AJCC AMERICAN JOURNAL OF CRITICAL CARE, March 2020, Volume 29, No. 2 135 Table Actions taken by physicians in response to patients’ reports of respiratory distress Percentage of 36 nurses who responded that physicians would … Frequency Request vital signs and/or oxygen saturation Always 56 Usually Order laboratory or imaging studies Order an intervention to relieve dyspnea Evaluate the patient Request that nurses reassess the patient later Take none of these actions 3 14 33 53 3 39 39 33 42 28 0 Half the time 3 47 47 22 11 8 Seldom 0 8 6 3 8 25 Never 3 3 0 0 0 61 the ICU, most patients cannot speak due to the ventilator or altered mental status . . . it is important to use nonverbal cues from the patient to assess.” • “Patients who are clearly labored sometimes say their breathing is ‘not bad, 3/10.’ This . . . is sometimes because at baseline their breathing is terrible or they just don’t realize how hard they are working to breathe, whether because of delirium or they just don’t realize.” Patients’ Ability to Rate Dyspnea Seventy percent of ICU nurses reported that patients give a meaningful rating for dyspnea at least half of the time, and 81% reported that patients give a meaningful rating for pain at least half of the time. In other words, nurses had slightly less confidence in patients’ dyspnea ratings than in their pain ratings. Interventions After Dyspnea Assessment For patients who report increasing shortness of breath, nearly all nurses (95%) said that they employ nonpharmacologic interventions such as repositioning techniques and coaching the patient to take slow, deep breaths. Many (60%) reported assessing the need for narcotics. Nearly all nurses (86%) said they notify a physician when shortness of breath increases, and 65% summon a respiratory therapist. Fifty-seven percent of nurses surveyed said it would be useful to have an algorithm with specific options for the treatment of dyspnea (eg, repositioning, facial fan, morphine). Nurses reported that physicians would always or usually take the following actions when their patients reported increased respiratory distress: request vital signs and/or oxygen saturation (95%), Most nurses found the dyspnea assessment tool easy to administer and noted that using it did not interfere with workflow. 136 order laboratory or imaging studies (42%), order a pharmacologic or nonpharmacologic intervention to relieve dyspnea (47%), evaluate the patient (75%), or request that nurses reassess the patient later (81%). Rarely (3% of the time), nurses reported that the physician responsible would take none of these actions (see Table). Discussion Our data show that most ICU nurses feel it is important to routinely assess and document dyspnea. Most nurses in our study found that the single-dimension scale was easy to use and did not impede workflow. We found 3 areas for possible improvement. (1) Descriptive terms used to ask patients to rate their dyspnea are not uniform. (2) Nurses reported frequently asking a yes/no question (eg, “Are you having shortness of breath?”) and recording a response of no as a 0 rating rather than asking the patient for a rating. (3) Nurses reported frequently using observed signs to modify or supplant the patient’s rating. Importance of Dyspnea Assessment Consistent with the results of our earlier survey of medical-surgical nurses,20 most ICU nurses stated that measuring dyspnea with a standard tool and periodically documenting dyspnea are important. Nurses also agreed that routine assessment can improve care delivery and patients’ outcomes. Dyspnea in ICU patients is clearly correlated with suffering that may lead to long-term harmful sequelae, including posttraumatic stress disorder. Patients experiencing moderate to severe dyspnea during hospitalization may be at increased risk for negative outcomes.4 Many ICU nurses reported that they had always included dyspnea in their patient assessments but had not used a standard scale or routinely documented findings. Nurses reported that incorporating routine measurement is easy and that providing a standard entry on the electronic form could even improve workflow. AJCC AMERICAN JOURNAL OF CRITICAL CARE, March 2020, Volume 29, No. 2 www.ajcconline.org Downloaded from http://aacnjournals.org/ajcconline/article-pdf/29/2/132/125370/132.pdf by Agus wahyudi on 22 August 2020 • “In 10 www.ajcconline.org 9 8 Breathlessness rating 7 6 5 4 3 2 1 0 Patient report Nurse estimate Figure 4 Differences between patients’ reports of “breathlessness” and nurses’ estimates of breathlessness; data from Haugdahl et al.21 Patients undergoing spontaneous breathing trials were asked, “Do you have a sensation of breathlessness?” by using a scale of 0 to 10, with 0 indicating “no, not at all” and 10 indicating “yes, worst imaginable.” Nurses were asked to estimate the patient’s breathlessness by using the same scale. This figure shows the data for 62 patients who rated breathlessness 4 or greater, with corresponding nurses’ estimates (there were overlaps, eg, in 5 instances the patient rated dyspnea 5 and the nurse rated dyspnea 2). Bold dashed line indicates group mean. assessment of respiratory distress would provide a better way to document this disagreement. Nurses in our study felt that patients could provide meaningful dyspnea ratings nearly as often as meaningful pain ratings. This finding was very similar to our findings with medical-surgical nurses. When ICU nurses were concerned that a patient’s rating did not truly reflect the patient’s discomfort, they responded by asking further questions or rephrasing and by using objective findings to modify the patient’s report. Need for a Universal Dyspnea Assessment Tool Implementing routine assessment with a tool that is easy, fast, and inexpensive can lead to early recognition of deterioration in a patient’s status and subsequent interventions to improve symptom management. AJCC AMERICAN JOURNAL OF CRITICAL CARE, March 2020, Volume 29, No. 2 137 Downloaded from http://aacnjournals.org/ajcconline/article-pdf/29/2/132/125370/132.pdf by Agus wahyudi on 22 August 2020 Areas for Improvement Uniform Language. Although a widely used plainlanguage definition of dyspnea (breathing discomfort) exists, many nurses used other terms (eg, shortness of breath or breathing difficulty) when describing to patients what they should rate. This difference undoubtedly leads to more variance in the data, but no direct evidence shows whether this is an important problem in clinical measurements. Response of No Versus Rating of 0. Many nurses reported asking a yes/no question about dyspnea and recording responses of no as 0. It takes only a few seconds more to collect a rating from the patient, and pertinent information may be lost by using this shortcut. Patient’s Report Versus Nurse’s Observation. By definition, dyspnea is a patient’s own experience of breathing discomfort, so measuring dyspnea requires asking the patient. Only patients know how much discomfort they are experiencing, so a patient’s report of symptoms is often considered the gold standard. Several studies have shown that clinicians’ estimates of dyspnea are poorly correlated with patients’ reports (R2 values ranging from 0.2 to 0.4).6,8,21,22 Although these correlations may be statistically significant in populations, one can have little confidence in estimating the discomfort of a given patient. One study showed that in patients who reported a dyspnea rating of 4 or greater (on a scale of 0 to 10), 47% of nurses underestimated the patient’s dyspnea rating by at least 4 points (Figure 4).21 A reliable patient report is unavailable in some instances (eg, cognitively impaired or unresponsive patients). In these cases, nurses use their best alternative to fill the information gap and properly care for the patient. Although well intended, this method creates difficulty in interpreting the record. A comparison of the results of this study and those of our earlier study20 indicates that this problem is much more common in ICU patients, who are more likely to be impaired because of heavier sedation and more severe illness. Nurses who used physical signs to substitute for or modify the patient’s report did so 92% of the time because the patient was unresponsive (eg, sedated). We suggest that this information gap would be best documented by providing nurses with a separate scale to note their own assessment of respiratory distress, rather than by having nurses act as proxies for a patient’s report. Less commonly, nurses modified patients’ ratings because patients appeared more uncomfortable than their reports suggested (the nurses thereby erred on the side of providing improved symptom relief) or patients appeared less uncomfortable than their reports suggested (uncommon in our survey). A separate scale to note the clinician’s Treatment Practices Once dyspnea is recognized, management includes pharmacologic and nonpharmacologic interventions2,30 that are implemented while pursuing an accurate diagnosis so the underlying cause can be appropriately treated. Nurses readily reported using interventions such as repositioning; remaining with the patient; coaching slow, deep breathing and providing reassurance; and notifying the physician or respiratory therapist. Physicians often request closer monitoring, additional laboratory or imaging studies, and pharmacologic interventions. Most nurses surveyed (57%) reported that a treatment algorithm for acutely dyspneic patients would be useful. Study Limitations The nurses at our institution may not be representative of nurses at all hospitals. Ours is an academic 138 tertiary care hospital, and several of the attending physicians in our medical ICUs work closely with researchers in our dyspnea laboratory. These physicians may have influenced the level of dyspnea awareness among nurses and respiratory therapists. (Our sample was drawn about equally from medical and surgical ICUs.) Conclusion Implementation of dyspnea assessment and documentation in the ICU requires acceptance and support by the nurses who perform these assessments. A significant barrier to adoption of yet another nursing requirement is the perception that it will impede workflow, burden busy nurses, and cause resentment. Our study of front-line ICU nurses shows, on the contrary, that routine dyspnea measurement is feasible in the highly stressful critical care environment, that nurses were able to readily incorporate it into their practice, and that nurses endorse it as important to patient care. The Joint Commission established standards for pain assessment and intervention decades ago in response to the national report of undertreated pain. We believe that the same standards should exist for dyspnea. ACKNOWLEDGMENTS The authors are very grateful to the unit nurses for their enthusiastic participation, the Lois E. Silverman Department of Nursing for enabling and supporting this project, and Dr Robert W. Lansing for his generous time and valuable input. FINANCIAL DISCLOSURES This study was supported by NIH grant NR10006 to Robert B. Banzett. REFERENCES 1. Shih FJ, Chu SH. Comparisons of American-Chinese and Taiwanese patients’ perceptions of dyspnea and helpful nursing actions during the intensive care unit transition from cardiac surgery. Heart Lung. 1999;28(1):41-54. 2. Campbell ML. Dyspnea. Crit Care Nurs Clin North Am. 2017;29(4):461-470. 3. Schmidt M, Banzett RB, Raux M, et al. Unrecognized suffering in the ICU: addressing dyspnea in mechanically ventilated patients. Intensive Care Med. 2014;40(1):1-10. 4. Stevens JP, Baker K, Howell MD, Banzett RB. Prevalence and predictive value of dyspnea ratings in hospitalized patients: pilot studies. PLoS One. 2016;11(4):e0152601. 5. Pesola GR, Ahsan H. Dyspnea as an independent predictor of mortality. Clin Resp J. 2016;10(2):142-152. 6. Binks AP, Desjardin S, Riker R. ICU clinicians underestimate breathing discomfort in ventilated subjects. Respir Care. 2017; 62(2):150-155. 7. Schmidt M, Demoule A, Polito A, et al. Dyspnea in mechanically ventilated critically ill patients. Crit Care Med. 2011; 39(9): 2059-2065. 8. Puntillo KA, Arai S, Cohen NH, et al. Symptoms experienced by intensive care unit patients at high risk of dying. Crit Care Med. 2010;38(11):2155-2160. 9. de Miranda S, Pochard F, Chaize M, et al. Postintensive care unit psychological burden in patients with chronic obstructive pulmonary disease and informal caregivers: a multicenter study. Crit Care Med. 2011;39(1):112-118. 10. Cuthbertson BH, Hull A, Strachan M, Scott J. Post-traumatic stress disorder after critical illness requiring general intensive care. Intensive Care Med. 2004;30(3):450-455. AJCC AMERICAN JOURNAL OF CRITICAL CARE, March 2020, Volume 29, No. 2 www.ajcconline.org Downloaded from http://aacnjournals.org/ajcconline/article-pdf/29/2/132/125370/132.pdf by Agus wahyudi on 22 August 2020 Intensive care unit nurses strongly endorsed the use of a standard tool to measure dyspnea and to record and track it at every shift. The 0-to-10 numeric scale was chosen for its brevity and ease of use, for its consistency with the common pain assessment tool, and because 10-point scales are broadly recognized and understood by the general population. Other assessment scales exist and can provide a much richer collection of data23,24 but are more cumbersome to use and thus may not gain acceptance for routine screening in the busy inpatient setting. Nurses in focus sessions indicated that a simpler tool may be easier for patients to comprehend; further studies to compare such scales may be useful. Because nurses and physicians evaluating dyspnea on the basis of physical signs nearly always underestimate the patient’s reported dyspnea,21 a uniform, systematic tool to evaluate signs of dyspnea in nonverbal patients would be useful. The Respiratory Distress Observation Scale is a recently developed instrument for the behavioral assessment of respiratory distress.25 This tool is intended for use only in patients who are unable to communicate. Validation trials in patients able to provide a dyspnea rating have shown a statistically significant correlation; at best the Respiratory Distress Observation Scale explains about half the variance in patients’ ratings (ie, R2 values generally ranging from 0.4 to 0.5 but sometimes ranging as low as 0.1).25-28 A modified version has been developed for ICU patients.29 The Respiratory Distress Observation Scale and other observation scales may prove to be acceptable surrogates for dyspnea ratings in patients unable to report but require further psychometric testing in ICU patients unable to report. 21. Haugdahl HS, Storli SL, Meland B, Dybwik K, Romild U, Klepstad P. Underestimation of patient breathlessness by nurses and physicians during a spontaneous breathing trial. Am J Respir Crit Care Med. 2015;192(12):1440-1448. 22. Hayes AW, Philip J, Spruyt OW. Patient reporting and doctor recognition of dyspnoea in a comprehensive cancer centre. Intern Med J. 2006;36(6):381-384. 23. Banzett RB, O’Donnell CR, Guilfoyle TE, et al. Multidimensional Dyspnea Profile: an instrument for clinical and laboratory research. Eur Respir J. 2015;45(6):1681-1691. 24. Yorke J, Moosavi SH, Shuldham C, Jones PW. Quantification of dyspnoea using descriptors: development and initial testing of the Dyspnoea-12. Thorax. 2010;65(1):21-26. 25. Campbell ML, Templin T, Walch J. A respiratory distress observation scale for patients unable to self-report dyspnea. J Palliat Med. 2010;13(3):285-290. 26. Hui D, Morgado M, Vidal M, et al. Dyspnea in hospitalized advanced cancer patients: subjective and physiologic correlates. J Palliat Med. 2013;16(3):274-280. 27. Chan YH, Wu HS, Yen CC, Campbell ML. Psychometric evaluation of the Chinese Respiratory Distress Observation Scale on critically ill patients with cardiopulmonary diseases. J Nurs Res. 2018;26(5):340-347. 28. Zhuang Q, Yang GM, Neo SH, Cheung YB. Validity, reliability, and diagnostic accuracy of the Respiratory Distress Observation Scale for assessment of dyspnea in adult palliative care patients. J Pain Symptom Manage. 2019;57(2):304-310. 29. Persichini R, Gay F, Schmidt M, et al. Diagnostic accuracy of respiratory distress observation scales as surrogates of dyspnea self-report in intensive care unit patients. Anesthesiology. 2015;123(4):830-837. 30. Booth S, Burkin J, Moffat C, Spathis A. Managing Breathlessness in Clinical Practice. London, England: Springer; 2014. Downloaded from http://aacnjournals.org/ajcconline/article-pdf/29/2/132/125370/132.pdf by Agus wahyudi on 22 August 2020 11. Schelling G. Effects of stress hormones on traumatic memory formation and the development of posttraumatic stress disorder in critically ill patients. Neurobiol Learn Mem. 2002; 78(3):596-609. 12. Abidov A, Rozanski A, Hachamovitch R, et al. Prognostic significance of dyspnea in patients referred for cardiac stress testing. N Engl J Med. 2005;353(18):1889-1898. 13. Bøtker MT, Stengaard C, Andersen MS, et al. Dyspnea, a highrisk symptom in patients suspected of myocardial infarction in the ambulance? A population-based follow-up study. Scand J Trauma Resusc Emerg Med. 2016;24:15. 14. Djärv T, Metcalfe C, Avery KN, Lagergren P, Blazeby JM. Prognostic value of changes in health-related quality of life scores during curative treatment for esophagogastric cancer. J Clin Oncol. 2010;28(10):1666-1670. 15. Healy LA, Ryan AM, Moore J, et al. Health-related quality of life assessment at presentation may predict complications and early relapse in patients with localized cancer of the esophagus. Dis Esophagus. 2008;21(6):522-528. 16. Stevens J, Dechen T, Sheridan A, et al. Patient mortality, readmissions, and resource use associated with dyspnea among hospitalized patients [abstract 4921]. Presented at: American Thoracic Society International Conference; May 22, 2018; San Diego, CA. 17. Parshall MB, Schwartzstein RM, Adams L, et al; American Thoracic Society Committee on Dyspnea. An official American Thoracic Society statement: update on the mechanisms, assessment, and management of dyspnea. Am J Respir Crit Care Med. 2012;185(4):435-452. 18. Baker DW. Joint Commission statement on pain management. The Joint Commission website. https://www.jointcommission .org/joint_commission_statement_on_pain_management/. Published April 18, 2016. Accessed June 7, 2019. 19. Lush MT, Janson-Bjerklie S, Carrieri VK, Lovejoy N. Dyspnea in the ventilator-assisted patient. Heart Lung. 1988; 17(5):528-535. 20. Baker KM, DeSanto-Madeya S, Banzett RB. Routine dyspnea assessment and documentation: nurses’ experience yields wide acceptance. BMC Nurs. 2017;16:3. To purchase electronic or print reprints, contact American Association of Critical-Care Nurses, 101 Columbia, Aliso Viejo, CA 92656. Phone, (800) 899-1712 or (949) 362-2050 (ext 532); fax, (949) 362-2049; email, [email protected]. C E 1.0 Hour Category A Notice to CE enrollees: This article has been designated for CE contact hour(s). The evaluation demonstrates your knowledge of the following objectives: 1. Identify why patients who report dyspnea are at increased risk of adverse outcomes, including higher mortality rates in the hospital. 2. Describe how routine dyspnea assessment can lead to early recognition of a patient’s clinical decline and improve symptom management. 3. Recognize that nurses and physicians evaluating dyspnea on the basis of clinical signs routinely underestimate patients’ reports of dyspnea. To complete the evaluation for CE contact hour(s) for this article #A2029022, visit www.ajcconline.org and click the “CE Articles” button. No CE evaluation fee for AACN members. This expires on March 1, 2023. The American Association of Critical-Care Nurses is accredited as a provider of nursing continuing professional development by the American Nurses Credentialing Center’s Commission on Accreditation, ANCC Provider Number 0012. AACN has been approved as a provider of continuing education in nursing by the California Board of Registered Nursing (CA BRN), CA Provider Number CEP1036, for 1.0 contact hour. www.ajcconline.org AJCC AMERICAN JOURNAL OF CRITICAL CARE, March 2020, Volume 29, No. 2 139 Supplement Dyspnea survey questions and nurses’ responses Question Where do you currently work? MICU/SICU MICU A MICU B SICU NSICU TSICU CCU CVICU 5 2 3 8 1 7 6 5 34 1 1 What is your age? (optional) <25 26-30 31-35 36-40 41-45 46-50 51-55 56-60 61-65 No response 2 13 2 5 4 2 2 2 1 3 What ethnicity do you identify with? (optional) Hispanic or Latino Non-Hispanic or Latino No response 0 29 6 What race do you identify with? (optional) Indian/Alaska native Native Hawaiian/Pacific Islander Asian Black or African American White Other No response 0 0 2 0 30 0 4 How many years have you worked as an ICU nurse? <1 1-3 4-6 7-9 >10 2 9 7 2 17 How many years have you worked as an ICU nurse at BIDMC? <1 1-3 4-6 7-9 >10 5 13 2 3 14 No. of responses Question How important is it to use a uniform tool to assess for dyspnea? Very important 7 Important 19 Moderately important Of little importance Not important 8 2 1 How important is it to track dyspnea every shift? Very important Important Moderately important Of little importance Not important 16 16 4 1 0 How often is your assessment of the severity of respiratory distress meaningfully less than the patient’s rating of dyspnea? Always 90% of the time 80% of the time 70% of the time 60% of the time 50% of the time 40% of the time 30% of the time 20% of the time 10% of the time Never 3 0 3 1 0 7 4 4 6 3 6 How often is your assessment of the severity of respiratory distress meaningfully greater than the patient’s rating of dyspnea? Always 90% of the time 80% of the time 70% of the time 60% of the time 50% of the time 40% of the time 30% of the time 20% of the time 10% of the time Never 2 1 3 5 1 9 5 4 4 2 1 How important is the addition of routine dyspnea assessment in improving patient-centered care? Very important Important Moderately important Of little importance Not important 8 19 5 4 1 How important is the addition of routine dyspnea assessment in predicting adverse patient outcomes? Very important Important Moderately important Of little importance Not important 9 17 5 6 0 Continued Downloaded from http://aacnjournals.org/ajcconline/article-pdf/29/2/132/125370/132.pdf by Agus wahyudi on 22 August 2020 What gender do you identify with? (optional) Female Male No response No. of responses Supplement Continued Question No. of responses 0 3 24 10 How has the implementation of routine dyspnea assessment affected your workflow? Very positively Positively No effect Negatively Very negatively 1 11 25 0 0 In your opinion, would it be useful to have an algorithm with specific options for the treatment of dyspnea? (eg, repositioning, facial fan, morphine) Very useful Somewhat useful Not useful Unsure 3 18 13 3 Which of the following words or phrases do you use to explain to the patient what they are supposed to rate? (Please check all that apply) Short of breath Dyspnea Breathing discomfort Difficulty breathing/trouble breathing Can’t catch your breath None of the above 27 4 24 34 21 0 Some nurses begin symptom assessment by asking the patient a yes/no question, for instance “are you feeling any breathing discomfort.” A) Do you first ask a yes/no question? Yes No 28 9 B) If the patient responds “no,” do you document “0” without asking the patient to provide a number rating? Yes No 14 19 In my opinion, patients give a meaningful number rating for pain? Always 90% of the time 80% of the time 70% of the time 60% of the time 50% of the time 40% of the time 30% of the time 20% of the time 10% of the time Never 0 4 12 4 2 8 3 2 2 0 0 In my opinion, patients give a meaningful number rating for dyspnea? Always 90% of the time 80% of the time 70% of the time 60% of the time 50% of the time 40% of the time 30% of the time 20% of the time 10% of the time Never 1 4 8 3 3 7 3 2 3 3 0 Do you find it helpful to have standard words (none, mild, moderate, severe, unbearable) alongside the number scale to help communicate with patients who have difficulty using a number scale? Yes Uncertain No 24 8 5 Do you think it would be helpful to have a pictorial scale to help communicate with patients who have difficulty using a number scale? Yes Uncertain No 14 12 11 When you use physical signs to assess respiratory distress, what signs do you use? Tachypnea Difficulty speaking Accessory muscle use Heart rate Nasal flaring Restless movements Fearful facial expression Ventilator dyssynchrony 35 35 36 32 32 33 27 29 How often do you use only the patient’s report to provide a number for dyspnea? Always 90% of the time 80% of the time 70% of the time 60% of the time 50% of the time 40% of the time 30% of the time 20% of the time 10% of the time Never 6 3 3 1 0 9 1 1 2 1 9 Continued Downloaded from http://aacnjournals.org/ajcconline/article-pdf/29/2/132/125370/132.pdf by Agus wahyudi on 22 August 2020 How easy or difficult is it to administer the dyspnea assessment? Very difficult Difficult Easy Very easy No. of responses Question Supplement Continued Question No. of responses Question No. of responses 34 25 25 13 When you report a patient’s dyspnea rating to the physician responsible for the patient… A) The physician requests vital signs and/or oxygen saturation. Always Usually Half the time Seldom Never 20 14 1 0 1 3 2 2 0 3 10 0 4 2 1 9 A) What are your reasons for using physical signs rather than patient report? (Select all that apply) Patient is unresponsive (eg, sedated) Patient is unable to use number scale Patient seems more uncomfortable than they claim Patient seems less uncomfortable than they claim 12 4 4 2 How often do you combine the patient’s report with observed physical signs of respiratory distress to provide a number for dyspnea? Always 90% of the time 80% of the time 70% of the time 60% of the time 50% of the time 40% of the time 30% of the time 20% of the time 10% of the time Never B) The physician orders laboratory or imaging studies. Always Usually Half the time Seldom Never 1 14 17 3 1 15 3 3 4 1 2 1 1 2 0 4 C) The physician orders an intervention to relieve dyspnea (pharmacologic or nonpharmacologic) Always Usually Half the time Seldom Never 5 12 17 2 0 In your opinion would it be useful to have a separate scale for RNs to record their observations of respiratory distress? Yes No D) The physician evaluates the patient. Always Usually Half the time Seldom Never 12 15 8 1 0 21 15 When your patient complains of increasing shortness of breath what are your actions? (Select all that apply) Coach slow, deep breathing Reposition Summon respiratory therapist Notify physician Provide facial fan 35 35 24 32 11 E) The physician requests nursing to reassess the patient later. Always Usually Half the time Seldom Never 19 10 4 3 0 F) The physician takes none of these actions. Always Usually Half the time Seldom Never 1 0 3 9 22 Assess need for narcotics 22 Abbreviations: BIDMC, Beth Israel Deaconess Medical Center; CCU, coronary care unit; CVICU, cardiovascular intensive care unit; ICU, intensive care unit; MICU, medical intensive care unit; NSICU, neuroscience intensive care unit; RN, registered nurse; SICU, surgical intensive care unit; TSICU, trauma/surgical intensive care unit. Downloaded from http://aacnjournals.org/ajcconline/article-pdf/29/2/132/125370/132.pdf by Agus wahyudi on 22 August 2020 What are your reasons for using physical signs to substitute for or modify patient report? (Select all that apply) Patient is unresponsive (eg, sedated) Patient is unable to use number scale Patient seems more uncomfortable than they claim Patient seems less uncomfortable than they claim How often do you use only observed physical signs of respiratory distress to provide a number for dyspnea? Always 90% of the time 80% of the time 70% of the time 60% of the time 50% of the time 40% of the time 30% of the time 20% of the time 10% of the time Never