Uploaded by
common.user18405
Lifetime Risk of Stroke and Dementia: Framingham Study Estimates
advertisement

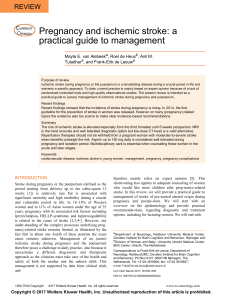
Personal View Lifetime risk of stroke and dementia: current concepts, and estimates from the Framingham Study Sudha Seshadri, Philip A Wolf Lancet Neurol 2007; 6: 1106–14 Department of Neurology, Boston University School of Medicine, Boston, Massachusetts and the NHLBI’s Framingham Heart Study, Framingham, MA, USA (S Seshadri MD, PA Wolf MD) Correspondence to: S Seshadri, Department of Neurology, Boston University School of Medicine, 715 Albany Street, B-602, Boston, MA 02118-2526, USA [email protected] 1106 The main neurological causes of morbidity and mortality are stroke and dementia. We contend that the most relevant and readily communicated risk estimate for stroke and dementia is lifetime risk, which is the probability of someone of a given age and sex developing a condition during their remaining lifespan. Lifetime risk estimates describe the population burden; however, they can be refined with risk-stratified models to enable individual risk prediction. Community-based data on a group of North Americans of European descent indicate that the lifetime risk of stroke for a middle-aged woman is 1 in 5 and for a middle-aged man is 1 in 6. The lifetime risk of stroke was equal to the lifetime risk of dementia and equal to or greater than the lifetime risk of Alzheimer’s disease (1 in 5 and 1 in 10 for women and men, respectively), and the lifetime risk of stroke or dementia was greater than 1 in 3. Thus, the lifetime burden attributable to common neurological disease is immense. Introduction In the past century, the worldwide average life expectancy at birth rose sharply from less than 40 years in 1900 to more than 65 years in 1975; more of the population now live to be 80 years or older. A corollary of increased life expectancy is an increase in the individual and population burden of age-related diseases. Stroke and dementia are the most widely feared age-related neurological diseases, and are also the only neurological disorders listed in the ten leading causes of disease burden.1 Stroke is the third highest cause of mortality and the highest neurological cause of disability-adjusted life-years lost in the developed world; in developing countries that have a low overall mortality rate, stroke ranks second in disability-adjusted life-years lost.1 The 2007 statistical update from the American Heart Association estimates the lifetime risk of stroke and other cardiovascular diseases on the basis of data from the Framingham Heart Study.2 But what is the lifetime risk of a disease, and do we need this additional descriptive statistic for stroke when we already have the widely used measures of incidence, prevalence, relative risk, and cause-specific mortality? People should be aware of the risk of a disease at some point in their life; similarly, such statistics are essential for public health planners to estimate the projected disease burden in a population during its expected lifespan. The estimation of lifetime risk enables a longterm perspective, which is particularly important for conditions such as stroke where exposure to risk factors in midlife can alter the incidence of disease later.3 The lifetime risk of a condition can be defined as the probability that a person who is currently free of the condition will acquire it at some time during the remainder of their expected lifespan. The concept of lifetime risk was pioneered by cancer epidemiologists4–6 and later extended to chronic bone7 and mental health disorders.8 The term lifetime risk was used to describe the diagnosis of a specific disease (such as breast cancer5 or Alzheimer’s disease [AD]9), a specific disease event (such as hip fracture10 or stroke11), or the development of a risk factor (such as hypertension12 or obesity13). Lifetime risk was used to define risk from birth14 or, more frequently, to define the residual or remaining lifetime risk from an age when that risk becomes of relevance and of concern to a person or to a society, such as the remaining lifetime risk (or the lifetime risk) of breast cancer in adults, the risk of stroke from age 55 years, or the risk of dementia from age 65 years. The concept of lifetime risk is underused. Most neuroepidemiological papers address disease incidence and prevalence but do not provide any estimate of the lifetime risk of the condition in their study samples. In this Personal View, we present a conceptual definition of lifetime risk and distinguish it from measures of cumulative incidence and prevalence. We describe how the lifetime risk can be operationally defined and computed, and discuss data on the lifetime risks of stroke, dementia, and AD from one well characterised, community-based sample. In addition, we discuss the use of such estimates for health planning, public education, and the prediction of a person’s risk. We also set out the reasons and preliminary evidence for the expected regional and temporal differences in lifetime risk, and summarise some of the available data on the lifetime risk of various neurological diseases. The lifetime risk estimates for other common age-related diseases, such as cancer and cardiovascular disease, are compared with the lifetime risk of neurological disorders. With this Personal View, we aim to persuade more investigators to use lifetime risk estimates. Why define the lifetime risk of a condition? A brief historical perspective that describes the development and application of lifetime risk in the context of the Framingham database might be helpful. We realised the usefulness of the concept of lifetime risk in the early 1990s when neurologists were grappling with a simultaneously exciting and yet disappointing observation. An unexpected new risk factor—the apolipoprotein E (APOE) ε4 allele—was found to have a powerful effect on the age of onset and risk of AD in familial and apparently sporadic late-onset variants of the http://neurology.thelancet.com Vol 6 December 2007 Personal View What is the lifetime risk of a disease? The lifetime risk of a disease is clearly not synonymous with the age-specific annual incidence of the disease because lifetime risk is the risk over a long period rather than the risk over a year. The lifetime risk differs from conventional estimates of cumulative incidence (or cumulative risk) whenever we regard a disease that is common—with a prevalence greater than 10%—or a group in which there is a high risk of competing events (typically death by a different cause) that remove people from the at-risk group.17 Although estimates of the theoretical cumulative risk assume that people who die of alternative causes would have developed the disease at the same rate as those who survive, estimates of the actual lifetime risk recognise that the risk of disease after death is zero. Therefore, people who are free of a disease when they die have, essentially, escaped the condition. The cumulative incidence or risk not adjusted for mortality is frequently appropriate when regarding the role of an aetiological factor in the cause of a disease, whereas the experienced lifetime risk is appropriate when regarding individual or population risk. The lifetime risk of a disease is not synonymous with the prevalence of a condition in the population, because people with the trait or disease commonly live for a shorter time than people without the condition; therefore, if a condition shortens life expectancy, estimates of disease prevalence in a community underestimate the true lifetime risk. Finally, the lifetime risk does not assume that all people live to the upper age limit used in the risk calculation; rather, it weights each age interval on the basis of the actual probability that a person will live for that period. How can we estimate the lifetime risk? Operationally, the lifetime risk or, more accurately, the mortality-adjusted residual or remaining lifetime risk at any age is the conditional probability of developing a disease when a person has reached the baseline (index) age and is free of that disease. The conditional probability can be estimated on the basis of the mean age-adjusted incidence of the disease and the average residual life expectancy for each sex at a particular age. In 1994, when we first approached this question, there were lifetime risk estimates for breast cancer5 and hip fracture10 but http://neurology.thelancet.com Vol 6 December 2007 25 Men: all causes Men: ischaemic stroke Women: all causes Women: ischaemic stroke 20 Lifetime risk (%) disease.15 However, the allele is neither necessary nor sufficient to cause AD; rather, the APOE ε4 allele multiplied the underlying risk of the disease. A definition of a meaningful baseline or a priori risk—ie, the risk in all people before they were genotyped for APOE—is needed to put this risk in perspective. But what is an appropriate a priori risk estimate? Clearly, someone who is disease-free but feels at risk (eg, a 65 year old) would not want to know his or her risk only during the next year, or even during the next 5 years; rather, they would want to know the risk of ever getting the disease.4,16 15 10 5 0 55 65 75 Age (years) 85 95 Figure 1: Lifetime risk of all-cause stroke and ischaemic stroke from age 55 years Lifetime risk of first-ever stroke in Framingham Study participants (women and men) who were stroke-free at 55 years old and were followed during their lifespan. Adapted with permission from the American Heart Association.11 few reports of the lifetime risk for any of the common neurological diseases. Two notable exceptions were reports that estimated the lifetime risk of AD in high-risk families18 and a single report on the remaining morbid lifetime risk of AD in a community-based group.19 These and other studies that address the lifetime risk of nonneurological disorders used a double-decrement life-table method, which combined published life-expectancy data (mostly comprising national rather than group-specific data) and group-specific, observed disease-incidence data to estimate the lifetime risk. Because factors that affect disease incidence might also affect the risk of death by other causes, we concluded that disease incidence and mortality estimates from the same population would be preferable. The computational technique used to run these analyses has been described in detail.20 We were able to use these methods to estimate the lifetime risk of dementia and AD during 1997 and, more recently, we have estimated the lifetime risk of stroke and compared this with updated estimates of the lifetime risk of dementia and AD.9,11 What is the lifetime risk of stroke? The Framingham Study has prospectively screened participants for incident stroke since the original group was enrolled in 1948–50.21–23 With data from the 4897 original participants in the Framingham Study who were stroke-free and dementia-free at 55-years-old, 875 incident strokes were recorded during a follow-up period of up to 51 years (115 146 person-years); therefore, we estimated that the average 55-year-old man has a 1 in 6 risk of stroke during his lifetime, whereas the risk for an average 55-year-old woman is 1 in 5 (figure 1, table 1).11 Thus, women are more likely to have a stroke because of their greater life-expectancy: women had an 18% lifetime risk 1107 Personal View N* First stroke all-causes (875) First ischaemic stroke (749) Short-term and intermediate-term risks 10 year 20 year Lifetime risk Short-term and intermediate-term risks 30 year 10 year 20 year Lifetime risk 30 year Women 55 522 (448) 2·3 (1·7–2·9) 6·5 (5·6–7·5)† 14·3 (13·0–15·6) 21·1 (19·4–22·7)† 1·8 (1·3–2·3) 5·4 (4·5–6·2)† 12·1 (10·9–13·4) 18·1 (16·6–19·7)† 65 462 (400) 4·6 (3·8–5·5)† 13·2 (11·8–14·5) 19·5 (17·8–21·1)‡ 20·6 (19·0–22·3)† 3·9 (3·1–4·7)† 11·3 (10·1–12·6) 16·9 (15·4–18·5)‡ 17·9 (16·2–19·5)† 75 347 (303) 10·5 (9·1–11·9) 18·3 (16·5–20·1)† ·· 19·7 (17·8–21·6)† 9·1 (7·8–10·4) 16·0 (14·3–17·8)† 85 140 (123) 13·4 (11·1–15·6)† ·· 15·8 (13·3–18·2)† 11·9 (9·8–14·0)† ·· ·· ·· 17·2 (15·4–19·0)† ·· 13·8 (11·5–16·2)† Men 55 353 (301) 2·9 (2·2–3·6) 8·7 (7·5–9·9)† 14·7 (13·2–16·2) 16·9 (15·3–18·6)† 2·4 (1·7–3·1) 7·3 (6·2–8·4)† 12·6 (11·2–14·1) 14·5 (12·9–16·0)† 65 293 (251) 7·0 (5·8–8·2)† 14·1 (12·5–15·8) 16·5 (14·7–18·3)‡ 16·8 (15·1–18·6)† 5·8 (4·7–6·9) 12·3 (10·7–13·8) 14·1 (12·4–15·7)‡ 14·4 (12·8–16·1)† 75 166 (145) 10·4 (8·6–12·1) 12·0 (10·1–13·8)† 85 38 (30) 8·5 (5·7–11·3)† 13·8 (11·8–15·8)‡ ·· ·· 14·3 (12·2–16·4)† 9·3 (7·7–11·0) ·· 9·8 (6·7–12·8)† 6·6 (4·1–9·0)† ·· ·· 12·5 (10·6–14·4)† ·· 7·8 (5·0–10·6)† *All-cause stroke (ischaemic stroke). Risks shown as percentages (95% CI). Comparison of risks in men and women with z-test. †=p<0·01. ‡=p<0·05. Table 1: Age-specific and sex-specific mortality-adjusted 10-year, 20-year, 30-year, and lifetime risk estimates for the development of all-cause stroke and ischaemic stroke. Adapted with permission from the American Heart Association11 All-type dementia (400) Alzheimer’s disease (292) Short-term and intermediate-term risks 10 year 20 year Lifetime risk 30 year Short-term and intermediate-term risks 10 year 20 year Lifetime risk 30 year Women 65 1·0 (0·4–1·5) 7·6 (6·3–9·0) 75 7·4 (6·0–8·8) 20·6 (18·2–22·9) 85 20·3 (17·2–23·5) ·· 19·4 (17·2–21·6) 21·7 (19·3–24·0) 0·6 (0·1–1·0)* 5·4 (4·3–6·6)* ·· 23·1 (20·5–25·7) 5·4 (4·2–6·6)* 16·3 (14·2–18·5) ·· 24·3 (20·7–27·8) 16·9 (13·9–19·8) ·· 15·2 (13·2–17·2)* 17·2 (15·0–19·4)† ·· 18·5 (16·2–20·9) ·· 20·3 (17·0–23·6)† Men 65 1·6 (0·8–2·4) 7·7 (6·1–9·3) 75 7·6 (5·8–9·3) 14·2 (11·7–16·8) 85 13·8 (9·9–17·7) ·· 13·1 (10·9–15·3) 14·3 (12·0–16·7) 0·9 (0·3–1·5)* 4·4 (3·2–5·7)* ·· 15·8 (13·0–18·5) 4·4 (3·0–5·7)* 9·2 (7·1–11·3)* ·· 16·9 (12·5–21·4) 10·0 (6·6–13·4) ·· 8·3 (6·5–10·2)* 9·1 (7·2–11·1)* ·· 10·2 (7·9–12·5)* ·· 12·1 (8·2–15·9) Risks shown as percentages (95% CI). Comparison of risk of AD in corresponding age and sex categories with z-test. *=p<0·01. †=p<0·05. Table 2: Age-specific and sex-specific mortality-adjusted 10-year, 20-year, 30-year, and lifetime risk estimates for dementia and Alzheimer’s disease at index ages 65 years, 75 years, and 85 years. Adapted with permission from the American Heart Association.11 of ischaemic stroke at age 55, whereas the corresponding risk in men was 14% (p<0·01). Only one other report on the lifetime risk of stroke has been published, with estimates based on a 6-year follow-up of the Rotterdam Study sample. The investigators’ results were similar to ours: the lifetime risk of stroke was about 1 in 5 for men and women at age 55 years.24 These two studies had several strengths, including the prospective ascertainment of end-points with standardised clinical diagnostic criteria (the Framingham data were gathered over a period of 50 years) and the complete ascertainment of stroke and mortality in the same community-based group. However, these estimates are based on only the risk of overt stroke and not the additional burden of silent (covert) stroke.25 Consequently, the lifetime risk of stroke that we report might be an underestimate of the true burden of cerebrovascular disease. The severity of stroke can vary, and our lifetime risk estimates do not distinguish between the lifetime risk of disabling stroke and the lifetime risk of any stroke. 1108 However, we found no published data on this important question. Furthermore, when we tried to analyse stroke severity in our database, the answer was complex: disability after stroke depends on age at stroke, prestroke disability, the presence or absence of comorbid disorders (such as arthritis and heart disease), and how long after stroke the disability was assessed (30 days or 6 months).26,27 Moreover, the answer varied with the definition of disability and how it was measured. These complex issues are beyond the scope of this Personal View, but the lifetime risk of disabling stroke must be studied within population samples such as the Framingham Heart study. Lifetime risks of stroke versus dementia We compared the lifetime risks of stroke and dementia and noted that lifetime risk of stroke is greater than lifetime risk of AD until people reach an advanced age (~85 years old). We made this comparison because dementia, which is mostly due to AD, is the only other http://neurology.thelancet.com Vol 6 December 2007 Personal View Lifetime risks in women The greater life expectancy for women translates into a greater lifetime risk of several diseases, which is true not only for disorders that are known to affect women at least as frequently as men (such as AD) but is also true for vascular diseases (such as stroke), where premenopausal, endogenous oestrogen concentrations might protect women. The mean age of first stroke is later in women than it is in men;29–31 however, because the average adult now spends more than 25% of their life in the sixth or subsequent decades, and during this time the average woman is postmenopausal, the survival advantage translates into a higher lifetime burden of AD and stroke. Thus, women typically need more long-term disability care than men. A similar effect was shown when comparing the lifetime burden of cardiovascular disease in smokers and non-smokers; the latter developed cardiovascular disease at a later age but had an overall greater lifetime risk of these diseases.32 Patterns in lifetime risk estimates of disease During the past decade several investigators have extended the concept of estimating lifetime risks to various cardiac disorders, such as coronary heart disease,33 congestive heart failure,34 and atrial fibrillation.35 Lifetime risk estimates fall into two broad categories on the basis of the pathophysiology of the underlying disease. One group of diseases has a peak incidence within a given age group, with decreased age-specific incidence in older http://neurology.thelancet.com Vol 6 December 2007 25 Dementia Delayed dementia Lifetime risk (%) 20 15 10 5 0 65 70 75 80 85 90 95 Age (years) Figure 2: Lifetime risk of dementia for women aged 65 years Actual (blue line) lifetime risk in 65-year-old, dementia-free women in the Framingham Heart Study11 who were followed up throughout their remaining life compared with projected lifetime risk (red line) of incident dementia if it could be delayed in all cases by 5 years (arrows). 25 Stroke all-causes Alzheimer’s disease 20 Lifetime risk (%) neurological disorder listed in the ten leading causes of total disease burden in developed countries, and these are the two most widely feared age-related neurological disorders in the public perception. A group of 2794 participants without dementia in the Framingham Study who were 65 years or older were followed up for a maximum of 29 years (42 233 person-years). There were 400 cases of incident dementia of all types and 292 cases of incident AD. We estimated the lifetime risk of any dementia at more than 1 in 5 in women and 1 in 6 in men, and the lifetime risk of AD at about 1 in 5 for women and 1 in 10 for men (table 2).11 A greater risk of dementia in women was also noted in the Rotterdam study, which reported a 33% lifetime risk of dementia in women compared with a 16% lifetime risk in men.28 Our projections suggest that, assuming a constant life expectancy, if the age at onset of clinical dementia could be delayed in all cases by just 5 years, the lifetime risk of dementia could be drastically reduced (figure 2). The lifetime risk of stroke was greater than the lifetime risk of AD for men and women at ages 55 years, 65 years, and 75 years; only men and women aged 85 years or older had a greater lifetime risk of AD than stroke (figure 3).11 The realisation that the lifetime risk of stroke or dementia was more than 1 in 3 in both sexes, which is higher than the lifetime risk of coronary heart disease in women, is sobering.7 15 10 5 0 Women 65 years Women 75 years Women 85 years Men 65 years Men 75 years Men 85 years Figure 3: Comparison of lifetime risks for stroke and Alzheimer’s disease Simple educational charts of the lifetime risks of developing stroke and dementia in men and women at ages 65 years, 75 years, and 85 years on the basis of data from the Framingham Heart Study.11 people. For these diseases, the lifetime risk estimates also peak at a specific age (not always the age with the greatest annual age-specific incidence) and either flatten or decline thereafter.36,37 This levelling of risk appears to occur for breast cancer, coronary artery disease, and stroke, although a definite decline might not always be reported. For other diseases and traits that are thought to be related to ageing, per se, such as congestive heart failure and AD, current life expectancies are associated with an increase in age-specific incidence with increasing age, which almost exactly matches and counterbalances the decline in remaining life expectancy. Hence, the estimated lifetime risk is fairly constant, which enables the generation of a single risk estimate that is applicable 1109 Personal View 25 HTN stage 2 HTN stage 1 preHTN Normal BP Lifetime risk (%) 20 15 10 5 0 65 70 75 80 Age (years) 85 90 95 Figure 4: Lifetime risk of stroke for men, stratified by JNC7 blood pressure categories Lifetime risk of stroke for men aged 65 years by baseline blood pressure category. Four blood pressure categories were defined, with SBP and DBP values measured in mm Hg and cut-off points similar to those used by JNC7. Green line: normal BP=SBP <120 and DBP <80. Dark blue line: preHTN=SBP >120 but <140 and/or DBP >80 but <90. Red line: HTN stage 1=SBP >140 but <160 and DBP >90 but <100. Light blue line: HTN stage 2=SBP >160 and/or DBP >100. HTN=hypertension. SBP=systolic blood pressure. DBP=diastolic blood pressure. preHTN=prehypertension. JNC=Joint National Committee on Prevention, Detection, and Evaluation of Treatments of High Blood Pressure. Adapted with permission from the American Heart Association.11 to the entire population of adults at risk. A relatively constant risk estimate for the lifetime risk of stroke is also found over a specified age range, for example 55–75 years (table 1, figure 3).11 Individualised risk prediction People who are apprehensive about the risk of a disabling and potentially fatal condition, such as a stroke, should be rightly concerned with not just the annual or 5-year risk, although these short-term risks are important, but also with the risk that they will develop the condition at any time in their life. Someone who is worried about the risk of stroke could use a predictive scale, such as the Framingham stroke risk profile, to predict the 10-year risk of stroke.31 However, risk prediction for the remaining lifespan of a 45–75 year old would certainly require estimation of risk over a period longer than 10 years; the lifetime risk estimates that we generated on this basis have been included in the most recent statistical update of the American Heart Association.2 However, there are several caveats with lifetime risk estimates for individual risk prediction. First, these estimates are, by design, population estimates; for any individual risk, the estimated lifetime risk would vary with remaining life expectancy (eg, a family history of longevity or other underlying diseases), risk factor profile, and the success of risk factor management. Because disorders that increase the risk of stroke, such as atrial fibrillation or congestive heart failure, might alter overall life expectancy and increase the risk of dying by other causes, the change in lifetime risk of stroke associated with these risk factors is not intuitively predictable. 1110 Second, lifetime risk estimates do not distinguish between immediate and remote risks and, hence, should be combined with short-term risk estimates when counselling young people. Finally, the lifetime risk estimates we have generated tend to be unstable for people in the tenth decade and beyond because estimates for people older than 90 years are based on small numbers. Nevertheless, lifetime risk estimates are useful for individual and mass-media education campaigns because they are easier to comprehend than alternative measures, such as incidence, prevalence, or relative risk. For example, when presented with information on annual stroke risk “many subjects struggled to understand the concept of cumulative risks”.38 Conversely, in the 1990s the American Cancer Society effectively used a single lifetime risk estimate of 1 in 9 to raise awareness of the risk of breast cancer in women.39 Bayesian techniques can be used to compute risk-factor-specific estimates of the lifetime risk of a disease: having one APOE ε4 allele doubled the age-specific and sex-specific risk of AD, whereas being APOE ε4 negative halved the basal agespecific and sex-specific risks.3 Individualised estimates of the lifetime risk of AD were presented to participants in the REVEAL (Risk Evaluation and Education for AD) study,40 and nearly half the participants could recall the figure a year later. The results of research into effective health communication suggest that patients prefer health risks to be framed in absolute terms, with bar graphs, and calculated over their expected lifetime.17 Risk-factorspecific lifetime risk estimates can also minimise psychological distress18 by directly linking risk estimates to an intervention that can favourably modify the estimates. Stroke risk prediction can be refined by including individual risk factors. For example, our data showed dramatic differences in the lifetime risk of stroke according to blood pressure level: lifetime risk of stroke in men with normal blood pressure (<120 mm Hg systolic and <80 mm Hg diastolic) is about half that of men with a baseline blood pressure in the hypertensive range (≥140 mm Hg systolic or ≥90 mm Hg diastolic), as assessed by the Seventh Joint National Committee on the Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (figure 4).41 For women, the corresponding risk fell from 1 in 4 in pateints with hypertension to 1 in 6 in patients who were normotensive. These data have been used to create simple and educational bar diagrams (figure 5). Nomograms and charts have been produced to present the lifetime risk of several late-life diseases, such as hip fractures, as a function of a risk factor estimate (bone density).42 We have used Framingham data on the lifetime risk of stroke and lifetime risk of all cardiovascular disease to produce charts and nomograms that estimate risk on the basis of individual risk factors, such as hypertension and diabetes,43 but further development of http://neurology.thelancet.com Vol 6 December 2007 Personal View 30 Blood pressure ≥140/90 Hg Blood pressure <120/80 Hg 25 20 Lifetime risk (%) risk-factor-specific lifetime risk estimates for stroke, as calculated for combined cardiovascular endpoints, is needed.44 However, the use of our risk-specific lifetime estimates compared with the older Framingham risk prediction scores and the interactive nomograms that have been widely used for years as effective educational, prognostic, and risk-stratification tools has not yet been directly assessed. We do not know how the presentation of lifetime risks rather than 10-year risks will alter risk perception and health-related behaviours. In theory, the lifetime risk is a useful tool to give middle-aged adults a long-term risk perspective. For this reason, a recent update of the Evidence-based Guidelines for Cardiovascular Disease Prevention in Women suggests an alteration to the “approach to risk stratification of women” that places “greater emphasis on lifetime risk than on short-term absolute risk.”44 15 10 Population differences in lifetime risk estimates Lifetime risk estimates are a useful public health tool that can be estimated in any population for which we have data on disease incidence and cause-specific mortality. More estimates of lifetime risk from racially, geographically, and socioeconomically diverse populations are needed because there are acknowledged differences in stroke incidence and life expectancy among ethnic groups, countries, and, possibly, socioeconomic groups.45–47 Lifetime risk can vary with the differences in life expectancy between developed and developing countries. Lifetime risk estimates have been used to categorise countries as high-risk or low-risk for hip fractures, and such categorisation can help health planning and budget allocation.48 Risk estimates are, however, only as good as the data used to calculate them, and under-reporting of events in developing countries can lead to underestimation of risk. Temporal trends in lifetime risk of stroke Lifetime risk is not static over time. Temporal trends in these risks should be expected because life expectancy rises or falls, the number of risk factors change, and as diagnostic criteria and the sensitivity of diagnostic tests for a condition change. With the Framingham data,32 we noted that there was a decreasing trend in the lifetime risk of stroke at age 65 years across the three periods analysed (1950–1977, 1978–1989, and later than 1990) that did not reach statistical significance for men or women.32 Because the age-adjusted annual incidence and 10-year cumulative incidence of stroke decreased over the same three periods, the stable lifetime risk is likely to be due to increases in life expectancy offsetting decreases in annual and shorter-term risks of stroke. Similar estimates are needed from other population samples because temporal trends in the lifetime risk of stroke can vary between countries and among different ethnic groups within a country. Thus, increased lifetime risk of stroke due to greater life expectancy is a particularly http://neurology.thelancet.com Vol 6 December 2007 5 0 Men Women Figure 5: Lifetime risks of stroke for men and women according to baseline blood pressure Simple educational bar graphs that show the lifetime risks of stroke in men and women with a BP of <120/80 mm Hg compared with the lifetime risks of stroke in men and women with a BP of >140/90 mm Hg.11 important issue in countries that are currently undergoing a rapid demographic transition, such as India and China. The results of the Auckland stroke study, which gathered incident stroke data through an ongoing stroke registry, suggested that although there was an overall decline in the incidence of first stroke of 14% (95% CI 12%–29%) between 1981 and 2002, there was a considerable (2·7-fold, 1·0-fold to 7·3-fold) increase in stroke incidence in Pacific islanders, which the authors attributed to an increase in the risk of obesity in this ethnic group.49,50 Lifetime risk of risk factors for stroke Lifetime risk estimates are a useful measure of risk factor burden in populations. For some of these reversible disorders, such as obesity and hypertension, the prevalence can change as people revert from a disease condition to a healthy state. However, people who have been exposed to these risk factors have an increased risk even after they revert to a healthy state.3 Studying the lifetime risk of developing risk factors for stroke and vascular disease, such as hypertension,12 obesity,13 hypercholesterolaemia,51 and diabetes,52,53 has helped to highlight the magnitude of the public health burden associated with these disorders. The study of lifetime risk has also shown the need to target societal factors and 1111 Personal View Disease or risk factor Index age (years) Men Women Stroke11 55 1/6 1/5 Dementia11 65 1/7 1/5 Alzheimer’s disease11 65 1/10 1/5 Parkinsonism55 65 1/25 1/25 Parkinson’s disease55 65 1/50 1/75 Stroke or dementia11 65 1/3 1/2 All cardiovascular disease43 40 2/3 >1/2 Coronary heart disease 40 1/2 1/3 Congestive heart failure57 40 1/5 1/5 Atrial fibrillation35 40 1/4 1/4 Breast5 40 1/1000 1/8 Prostate59 40 1/6 ·· Lung58 40 1/12 1/17 All58 40 1/4 1/5 50 1/20 1/6 Hypertension12 65 9/10 9/10 Type 2 diabetes 40 1/3 1/3 Obesity 40 1/3 1/3 Neurological Cardiovascular Cancers Other diseases or injuries Hip fracture10 Risk factors for stroke Selection is illustrative rather than comprehensive. Lifetime risk estimates from the Framingham study have been assessed with similar methods and are, therefore, comparable. However, variations in the data and methods used in the studies preclude a direct comparison of the lifetime risks of the other conditions listed. Table 3: Examples of lifetime risk for stroke and other disorders in people without the disorder at index age individual behaviours to reduce the lifetime risk of these apparently ubiquitous disorders. We have recently studied temporal trends in the prevalence and effect of stroke risk factors as an explanation for the observed decline in the age-specific incidence of stroke.54 The effect was explained by a decrease in the prevalence of some of the risk factors (such as high mean systolic blood pressure) and a decrease in the effect of other risk factors (such as atrial fibrillation). Lifetime risk of other neurological disorders The lifetime risks of other neurological conditions apart from stroke and dementia have been reported; these include Parkinson’s disease55 and carpal tunnel syndrome in people with diabetes.56 The lifetime risks of common neurological disorders have been compared with the risks of coronary heart disease and all cardiovascular diseases, the risks of common cancers (such as breast, prostate, and lung cancer) and all deaths from cancer, and with other age-related conditions, such as hip fractures, atrial fibrillation, and congestive heart failure (table 3).43,57–59 These data emphasise the enormity of the burden associated with common neurological diseases such as stroke and dementia. 1112 Search strategy and selection criteria References for this Personal View were identified by searches of PubMed from 1966 until August 25, 2007, with the terms “lifetime risk” and either “stroke” or “dementia”, which found 151 and 119 articles, respectively. Articles were also found by a review of all publications on the topics of “stroke” and “lifetime risk” from the Framingham Heart Study, through a review of citations in the primary articles and the Science Citation Index, and a review of articles that cited the identified articles. Finally, the authors searched their own files. Abstracts of all English language papers that met these criteria were reviewed to determine the relevance of their content, and 60 articles were studied in detail. Conclusions The lifetime risk of stroke, AD, or other disorders is an aggregate estimate of actual risk during the remaining lifespan that is applicable to people of a particular age and sex. The risk can be refined, however, for an individual on the basis of their risk factor profile. For an individual, the lifetinme risk is the appropriate a priori risk estimate to determine the usefulness and costeffectiveness of additional prognostic tests and algorithms. As multiple genetic, metabolic, imaging, and functional biomarkers for stroke and other neurological diseases are discovered we must understand their individual and collective value in risk prediction. Lifetime risk estimates for all cardiovascular diseases were published on the basis of an aggregate measure of midlife exposure to risk factors.60 Our future goals include the use of the Framingham data to develop a stroke risk profile that will provide lifetime risk estimates based on aggregate risk factor scores, which is a useful step towards evidence-based, personalised medicine. The lifetime risk of a disease can also be used as a population risk estimate to aid health economics and public policy decisions, to compare geographically or ethnically distinct populations, and to study temporal trends in disease risk in a population. The lifetime risk of stroke can be estimated for any population that has data on stroke incidence and non-stroke mortality; therefore, our recommendation is that studies that report stroke incidence should also provide lifetime risk estimates whenever possible. Contributors SS reviewed the literature, planned the outline of the Personal View, and drafted and critically revised the manuscript. PAW planned the outline of the Personal View and critically revised the manuscript. Both authors have read and approved the final version. Conflicts of interest We have no conflicts of interest. Acknowledgments We are supported by grants from the National Institute of Neurological Disorders and Stroke (NS17950), the National Institute of Aging (AG08122, AG16495), and the National Heart, Lung and Blood Institute’s Framingham Heart Study (NIH/NHLBI Contract # N01-HC-25195). http://neurology.thelancet.com Vol 6 December 2007 Personal View References 1 World Health Organization. Major burden of disease–leading 10 selected risk factors and leading 10 diseases and injuries in developed countries with low mortality levels. The World Health Report 2002 Statistical Annex, Annex 16 June 2007; Available at: http://www.who. int/whr/2002/annex/en/ (accessed January 12, 2006). 2 Rosamond W, Flegal K, Friday G, et al. Heart disease and stroke statistics—2007 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation 2007; 115: e69–171. 3 Seshadri S, Drachman DA, Lippa CF. Apolipoprotein E epsilon 4 allele and the lifetime risk of Alzheimer’s disease. What physicians know, and what they should know. Arch Neurol 1995; 52: 1074–79. 4 Cashman RE, Gerhardt PR, Goldberg ID, Handy VH, Levin ML. The probability of developing cancer. J Natl Cancer Inst 1956; 17: 155–73. 5 Feuer EJ, Wun LM, Boring CC, Flanders WD, Timmel MJ, Tong T. The lifetime risk of developing breast cancer. J Natl Cancer Inst 1993; 85: 892–97. 6 Bender AP, Punyko J, Williams AN, Bushhouse SA. A standard person-years approach to estimating lifetime cancer risk. The Section of Chronic Disease and Environmental Epidemiology, Minnesota Department of Health. Cancer Causes Control 1992; 3: 69–75. 7 Suman VJ, Atkinson EJ, O’Fallon WM, Black DM, Melton III LJ. A nomogram for predicting lifetime hip fracture risk from radius bone mineral density and age. Bone 1993; 14: 843–46. 8 Kramer M, von KM, Kessler L. The lifetime prevalence of mental disorders: estimation, uses and limitations. Psychol Med 1980; 10: 429–35. 9 Seshadri S, Wolf PA, Beiser A, et al. Lifetime risk of dementia and Alzheimer’s disease. The impact of mortality on risk estimates in the Framingham Study. Neurology 1997; 49: 1498–1504. 10 Melton III LJ. Lifetime risk of a hip fracture. Am J Public Health 1990; 80: 500–01. 11 Seshadri S, Beiser A, Kelly-Hayes M, et al. The lifetime risk of stroke: estimates from the Framingham Study. Stroke 2006; 37: 345–50. 12 Vasan RS, Beiser A, Seshadri S, et al. Residual lifetime risk for developing hypertension in middle-aged women and men: the Framingham Heart Study. JAMA 2002; 287: 1003–10. 13 Vasan RS, Pencina MJ, Cobain M, Freiberg MS, D’Agostino RB. Estimated risks for developing obesity in the Framingham Heart Study. Ann Intern Med 2005; 143: 473–80. 14 Bryant H. Breast cancer in Canadian women. BMC Women’s Health 2004; 4 (suppl 1): S12. 15 Corder EH, Saunders AM, Strittmatter WJ, et al. Gene dose of apolipoprotein E type 4 allele and the risk of Alzheimer’s disease in late onset families. Science 1993; 261: 921–23. 16 Drachman DA. If we live long enough, will we all be demented? Neurology 1994; 44: 1563–65. 17 Schouten LJ, Straatman H, Kiemeney LA, Verbeek AL. Cancer incidence: life table risk versus cumulative risk. J Epidemiol Community Health 1994; 48: 596–600. 18 Breitner JC. Clinical genetics and genetic counseling in Alzheimer’s disease. Ann Intern Med 1991; 115: 601–06. 19 Sayetta RB. Rates of senile dementia, Alzheimer’s type, in the Baltimore Longitudinal Study. J Chronic Dis 1986; 39: 271–86. 20 Beiser A, D’Agostino Sr RB, Seshadri S, Sullivan LM, Wolf PA. Computing estimates of incidence, including lifetime risk: Alzheimer’s disease in the Framingham Study. The Practical Incidence Estimators (PIE) macro. Stat Med 2000; 19: 1495–1522. 21 Dawber TR, Meadors GF, Moore FE, Jr. Epidemiological approaches to heart disease: the Framingham Study. Am J Public Health 1951; 41: 279–81. 22 Kannel WB, Dawber TR, McNamara PM. Vascular disease of the brain - epidemiologic aspects: the Framingham Study. Am J Public Health 1965; 55: 1355–66. 23 Wolf PA, Dawber TR, Thomas HE, Colton T, Kannel WB. Epidemiology of stroke. In: Thompson RA, Green JR, eds. Advances in neurology: stroke. New York: Raven Press, 1977. 5–19. 24 Hollander M, Koudstaal PJ, Bots ML, Grobbee DE, Hofman A, Breteler MM. Incidence, risk, and case fatality of first ever stroke in the elderly population. The Rotterdam Study. J Neurol Neurosurg Psychiatry 2003; 74: 317–21. http://neurology.thelancet.com Vol 6 December 2007 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 Leary MC, Saver JL. Annual incidence of first silent stroke in the United States: a preliminary estimate. Cerebrovasc Dis 2003; 16: 280–85. Guccione AA, Felson DT, Anderson JJ, et al. The effects of specific medical conditions on the functional limitations of elders in the Framingham Study. Am J Public Health 1994; 84: 351–58. Kelly-Hayes M, Wolf PA, Kannel WB, Sytkowski P, D’Agostino RB, Gresham GE. Factors influencing survival and need for institutionalization following stroke: the Framingham Study. Arch Phys Med Rehabil 1988; 69: 415–18. Ott A, Breteler MM, van HF, Stijnen T, Hofman A. Incidence and risk of dementia. The Rotterdam Study. Am J Epidemiol 1998; 147: 574–80. Wolf PA, Kannel WB, Verter J. Current status of risk factors for stroke. Neurol Clin 1983; 1: 317–43. Wolf PA, D’Agostino RB, Belanger AJ, Kannel WB. Probability of stroke: a risk profile from the Framingham Study. Stroke 1991; 22: 312–18. Carandang R, Seshadri S, Beiser A, et al. Trends in incidence, lifetime risk, severity, and 30-day mortality of stroke over the past 50 years. JAMA 2006; 296: 2939–46. Mamun AA, Peeters A, Barendregt J, Willekens F, Nusselder W, Bonneux L. Smoking decreases the duration of life lived with and without cardiovascular disease: a life course analysis of the Framingham Heart Study. Eur Heart J 2004; 25: 409–15. Lloyd-Jones DM, Larson MG, Beiser A, Levy D. Lifetime risk of developing coronary heart disease. Lancet 1999; 353: 89–92. Lloyd-Jones DM. The risk of congestive heart failure: sobering lessons from the Framingham Heart Study. Curr Cardiol Rep 2001; 3: 184–90. Lloyd-Jones DM, Wang TJ, Leip EP, et al. Lifetime risk for development of atrial fibrillation: the Framingham Heart Study. Circulation 2004; 110: 1042–46. Merrill RM, Kessler LG, Udler JM, Rasband GC, Feuer EJ. Comparison of risk estimates for selected diseases and causes of death. Prev Med 1999; 28: 179–93. Merrill RM, Weed DL. Measuring the public health burden of cancer in the United States through lifetime and age-conditional risk estimates. Ann Epidemiol 2001; 11: 547–53. Fuller R, Dudley N, Blacktop J. Older people’s understanding of cumulative risks when provided with annual stroke risk information. Postgrad Med J 2004; 80: 677–78. Segal M. Breast cancer complacency: he enemy of cure. http://www. fda.gov/bbs/topics/CONSUMER/CON00097.html (accessed September 22, 2007). Eckert SL, Katzen H, Roberts JS, et al. Recall of disclosed apolipoprotein E genotype and lifetime risk estimate for Alzheimer’s disease: the REVEAL Study. Genet Med 2006; 8: 746–51. Chobanian AV, Bakris GL, Black HR, et al. the seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure: the JNC 7 report. JAMA 2003; 289: 2560–72. Suman VJ, Atkinson EJ, O’Fallon WM, Black DM, Melton III LJ. A nomogram for predicting lifetime hip fracture risk from radius bone mineral density and age. Bone 1993; 14: 843–46. Lloyd-Jones DM, Leip EP, Larson MG, et al. Prediction of lifetime risk for cardiovascular disease by risk factor burden at 50 years of age. Circulation 2006; 113: 791–98. Mosca L, Banka CL, Benjamin EJ, et al. Evidence-based guidelines for cardiovascular disease prevention in women: 2007 update. Circulation 2007; 115: 1481–1501. Pickle LW, Mungiole M, Gillum RF. Geographic variation in stroke mortality in blacks and whites in the United States. Stroke 1997; 28: 1639–1647. Tolonen H, Mahonen M, Asplund K, et al. Do trends in population levels of blood pressure and other cardiovascular risk factors explain trends in stroke event rates? Comparisons of 15 populations in 9 countries within the WHO MONICA Stroke Project. World Health Organization monitoring of trends and determinants in cardiovascular disease. Stroke 2002 October; 33: 2367–75. Regional and racial differences in prevalence of stroke—23 states and District of Columbia, 2003. MMWR Morb Mortal Wkly Rep 2005; 54: 481–84. 1113 Personal View 48 49 50 51 52 53 54 1114 Kanis JA, Johnell O, De Laet C, Jonsson B, Oden A, Ogelsby AK. International variations in hip fracture probabilities: implications for risk assessment. J Bone Miner Res 2002; 17: 1237–44. Dyall L, Carter K, Bonita R, et al. Incidence of stroke in women in Auckland, New Zealand. Ethnic trends over two decades: 1981–2003. N Z Med J 2006; 119: U2309. Carter K, Anderson C, Hacket M, et al. Trends in ethnic disparities in stroke incidence in auckland, new zealand, during 1981 to 2003. Stroke 2006; 37: 56–62. Pencina MJ, D’Agostino RB, Beiser AS, Cobain MR, Vasan RS. Estimating lifetime risk of developing high serum total cholesterol: adjustment for baseline prevalence and single-occasion measurements. Am J Epidemiol 2007; 165: 464–72. Narayan KM, Boyle JP, Thompson TJ, Sorensen SW, Williamson DF. Lifetime risk for diabetes mellitus in the United States. JAMA 2003; 290: 1884–90. Narayan KM, Boyle JP, Thompson TJ, Gregg EW, Williamson DF. Effect of BMI on lifetime risk for diabetes in the USA. Diabetes Care 2007; 30: 1562–66. Seshadri S, Beiser A, Kelly-Hayes M, Kase CS, Kannel WB, Wolf PA. Is declining stroke incidence due to changes in risk factor prevalence or impact? Recalibrating the Framingham stroke risk profile to reflect temporal trends. Stroke 2007; 388: 481 (abstr). 55 56 57 58 59 60 Elbaz A, Bower JH, Maraganore DM, et al. Risk tables for parkinsonism and Parkinson’s disease. J Clin Epidemiol 2002; 55: 25–31. Singh R, Gamble G, Cundy T. Lifetime risk of symptomatic carpal tunnel syndrome in type 1 diabetes. Diabet Med 2005; 22: 625–30. Lloyd-Jones DM, Larson MG, Leip EP, et al. Lifetime risk for developing congestive heart failure: the Framingham Heart Study. Circulation 2002; 106: 3068–72. Stat bite: lifetime risk of being diagnosed with cancer. J Natl Cancer Inst 2003; 95: 1745. Merrill RM, Weed DL, Feuer EJ. The lifetime risk of developing prostate cancer in white and black men. Cancer Epidemiol Biomarkers Prev 1997; 6: 763–68. Lloyd-Jones DM, Dyer AR, Wang R, Daviglus ML, Greenland P. Risk factor burden in middle age and lifetime risks for cardiovascular and non-cardiovascular death (Chicago Heart Association Detection Project in Industry). Am J Cardiol 2007; 99: 535–40. http://neurology.thelancet.com Vol 6 December 2007