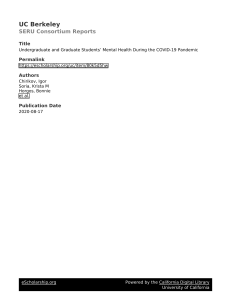
See discussions, stats, and author profiles for this publication at: https://www.researchgate.net/publication/284755217 Post-traumatic stress disorder Article in BMJ (online) · November 2015 DOI: 10.1136/bmj.h6161 CITATIONS READS 68 6,426 4 authors, including: Jonathan I Bisson Catrin Lewis Cardiff University Cardiff University 191 PUBLICATIONS 7,937 CITATIONS 26 PUBLICATIONS 598 CITATIONS SEE PROFILE SEE PROFILE Neil P Roberts Cardiff and Vale University Health Board 55 PUBLICATIONS 1,642 CITATIONS SEE PROFILE Some of the authors of this publication are also working on these related projects: Quality of psychosocial services in crisis View project Paradoxes and parallels: exploring the health implications of country vulnerability View project All content following this page was uploaded by Jonathan I Bisson on 29 March 2016. The user has requested enhancement of the downloaded file. BMJ 2015;351:h6161 doi: 10.1136/bmj.h6161 (Published 26 November 2015) Page 1 of 7 Clinical Review CLINICAL REVIEW Post-traumatic stress disorder Jonathan I Bisson professor of psychiatry, Sarah Cosgrove public representative, Catrin Lewis research psychologist, Neil P Roberts consultant clinical psychologist Division of Psychological Medicine and Clinical Neurosciences, School of Medicine, Cardiff University, Cardiff, UK What is post-traumatic stress disorder (PTSD)? PTSD is a mental disorder that may develop after exposure to exceptionally threatening or horrifying events. Many people show remarkable resilience and capacity to recover following exposure to trauma.1 PTSD can occur after a single traumatic event or from prolonged exposure to trauma, such as sexual abuse in childhood. Predicting who will go on to develop PTSD is a challenge.2 Patients with PTSD are at increased risk of experiencing poor physical health, including somatoform, cardiorespiratory, musculoskeletal, gastrointestinal, and immunological disorders.3 4 It is also associated with substantial psychiatric comorbidity,5 increased risk of suicide,6 and considerable economic burden.7 8 PTSD is a widely accepted diagnosis9 but some believe that the term medicalises understandable responses to catastrophic events and further disempowers those who are already disempowered.10 How common is PTSD? About 3% of the adult population has PTSD at any one time.11 Lifetime prevalence is between 1.9%12 and 8.8%,7 but this rate doubles in populations affected by conflict13 and reaches more than 50% in survivors of rape.5 How does PTSD present? Symptoms include persistent intrusive recollections, avoidance of stimuli related to the trauma, negative alterations in cognitions and mood, and hyperarousal (table⇓).14 15 A diagnosis can be made in someone whose ability to function normally has been noticeably impaired for one month according to DSM-5 criteria. Delayed presentation (sometimes years later) is common,7 including where the effects are severe.16 How is PTSD diagnosed? Box 1 describes the nature of the traumatic event(s) required by DSM-5 (diagnostic and statistical manual of mental disorders, fifth edition)14 for diagnosis and the proposed criteria by ICD-11 (international classification of diseases, 11th revision).17 Some events such as bullying, divorce, death of a pet, and learning about a diagnosis of cancer in a close family member are not deemed extreme enough to precipitate PTSD. However, they can result in almost identical symptoms and raise questions about the validity of the definitions for traumatic events.18 DSM-5 lists the 20 symptoms required for PTSD to be diagnosed,14 separated into four groups (table). All symptoms must be associated with the traumatic event. In the proposed criteria by ICD-11,17 PTSD will be diagnosed according to six criteria (table). To reflect the heterogeneity of PTSD, ICD-11 will introduce a new complex PTSD diagnosis (table). This requires satisfaction of the criteria for PTSD plus symptoms of mood dysregulation, negative self concept, and persistent difficulty in sustaining relationships and feeling close to others. Service users may meet the diagnostic criteria in one system but not in the other owing to the differences.19 Can PTSD be prevented? Psychological interventions Psychological interventions have been evaluated after traumas concerning a single incident, such as a road traffic crash and physical or sexual assaults. Meta-analyses show that brief, trauma focused, cognitive behavioural interventions can reduce the severity of symptoms when the intervention is targeted at those with early symptoms.20 21 However, non-targeted interventions (including psychoeducation, psychological debriefing, individual and group counselling, cognitive behavioural therapy (CBT) based programmes, and collaborative care based approaches) are largely ineffective.22-25 Drug interventions No robust evidence supports the use of drug interventions.26 Prevention after large scale traumatic events Evidence to support routine intervention after traumatic events involving many people (for example, terrorist attacks and natural disasters) is lacking. However, some evidence suggests that high levels of social support are perceived as protective.27 Consensus guidelines recommend supportive, practical, and Correspondence to: J I Bisson [email protected] For personal use only: See rights and reprints http://www.bmj.com/permissions Subscribe: http://www.bmj.com/subscribe BMJ 2015;351:h6161 doi: 10.1136/bmj.h6161 (Published 26 November 2015) Page 2 of 7 CLINICAL REVIEW What you need to know • Individual reactions to traumatic events vary greatly and most people do not develop a mental disorder after exposure to trauma • PTSD should be considered in any patient exposed to a major traumatic event • Up to 3% of adults has PTSD at any one time. Lifetime prevalence rates are between 1.9% and 8.8% • Psychological treatments, particularly trauma focused psychological therapies, can be effective • Although the effect sizes are not as high as for psychological therapies, drug treatments can be effective • Patients with complex PTSD should receive specialist multidisciplinary care Sources and selection criteria We identified Cochrane and other relevant systematic reviews and meta-analyses, and supplemented these with additional searches and our knowledge of the subject. Wherever possible, we used evidence from recent meta-analyses of randomised trials. Box 1 Traumatic event(s) required for diagnosis of PTSD DSM-5 criteria[14] Exposure to actual or threatened death, serious injury, or sexual violation, in one or more of the following ways: Directly experiencing the traumatic event(s) Witnessing traumatic event(s) in others Learning that the traumatic event(s) occurred to a close family member or close friend; cases of actual or threatened death must have been violent or unintentional Experiencing repeated or extreme exposure to aversive details of the traumatic event(s) (for example, first responders collecting human remains; police officers repeatedly exposed to details of child abuse); this does not apply to exposure through electronic media, television, movies, or pictures, unless this exposure is work related Proposed ICD-11 criterion[17] Exposure to an extremely threatening or horrific event or series of events pragmatic input but avoidance of formal clinical interventions unless indicated.28-30 Can PTSD be treated? Psychological therapy Clinical guidelines recommend trauma focused psychological therapies based on evidence from systematic reviews and meta-analyses.31-33 Individual trauma focused CBT and eye movement desensitisation and reprocessing (EMDR) (box 2) have been found to be equally effective.34 Group trauma focused CBT is also effective, but fewer studies have focused on this method.35 Non-trauma focused CBT—including components such as grounding techniques to manage flashbacks (for example, focusing on the here and now by describing items in a room), relaxation training (for example, controlled breathing and progressive muscle relaxation), positive thinking and self talk (for example, repeating positive phrases such as “I can deal with this”)—has been found to be superior to waiting list control groups and has shown similar efficacy to trauma focused CBT and EMDR immediately after treatment, but this is not maintained at follow-up.34 Non-trauma focused CBT offers a valid alternative to trauma focused therapy if the latter is poorly tolerated, contraindicated, or unavailable. It is unclear whether specific therapies are more or less effective for particular subgroups or trauma types.36 37 Research on interventions for more complex presentations of PTSD is limited.38 Evidence suggests that phased approaches may be beneficial for more complex presentations of PTSD.39 Phase based approaches target problems such as affect dysregulation, dissociation, and somatic symptoms to promote adaptive coping, a sense of safety, and stabilisation before undertaking any trauma focused intervention. For personal use only: See rights and reprints http://www.bmj.com/permissions Self help programmes Guided self help interventions for depression and anxiety disorders are being used as an alternative to face to face therapy as these interventions offer enhanced access to cost effective treatment.40 Some evidence suggests that internet based guided self help therapies effectively alleviate the symptoms of traumatic stress, but randomised controlled trials (RCTs) have historically been limited to subsyndromal populations.41 42 More recent evidence supports the efficacy of guided self help for people meeting diagnostic criteria for PTSD,43-45 but no head to head trials have compared guided self help with trauma focused psychological therapy administered by a therapist. Drug treatment The National Institute for Health and Care Excellence and World Health Organization recommend drug treatment second to trauma focused therapy.33 46 The effect sizes for drug treatments compared with placebo are inferior to those reported for psychological treatments with a trauma focus over waiting list or treatment as usual controls.33 47 Effect sizes with drug treatment are similar to those observed from use of antidepressants for depression compared with placebo.48 A recent systematic review and meta-analysis found statistically significant evidence (when at least two RCTs were available) of reduction in severity of PTSD symptoms for four drugs (fluoxetine, paroxetine, sertraline, and venlafaxine) versus placebo.47 In single RCTs, amitriptyline, GR205171 (a neurokinin-1 antagonist), mirtazapine, and phenelzine have shown superiority over placebo in reducing the symptoms of PTSD. In an RCT the α 1 adrenoceptor antagonist prazosin was found to reduce nightmares in veterans with PTSD,49 and a further RCT in veterans showed reduction in overall symptom severity.50 This suggests a possible role for α 1 adrenoceptor blockers in Subscribe: http://www.bmj.com/subscribe BMJ 2015;351:h6161 doi: 10.1136/bmj.h6161 (Published 26 November 2015) Page 3 of 7 CLINICAL REVIEW Box 2 Trauma focused exposure therapy, CBT and EMDR Exposure therapy • Therapists help patients to confront their traumatic memories through written or verbal narrative, detailed recounting of the traumatic experience, and repeated exposure to trauma related situations that were being avoided or evoked fear but are now safe (for example, driving a car where the road traffic incident occurred or walking in the busy park where an assault occurred) Cognitive therapy • Focuses on identifying and modifying misinterpretations that led patients to overestimate the current threat (for example, patients who think assault is almost inevitable if they leave the house) • Focuses on modifying beliefs and how patients interpret their behaviour during the trauma, including problems with guilt and shame EMDR • Standardised, trauma focused procedure. Involves the use of bilateral physical stimulation (eye movements, taps, or tones), hypothesised to stimulate the patient’s information processing to help integrate the targeted event as an adaptive contextualised memory PTSD, although further research is needed. Olanzapine, in contrast with another antipsychotic, risperidone, has been shown to accentuate the effects of antidepressants when resistance to treatment is encountered.51 52 Combination therapy Evidence to support the use of pharmacotherapy combined with psychological therapy over either treatment method separately is insufficient.53 How should PTSD and comorbidity be managed? PTSD is associated with depression, anxiety disorders, and drug and alcohol use disorders. Little evidence exists for the effectiveness of psychological interventions for PTSD with comorbid substance use disorders. Some evidence suggests that trauma focused CBT can be effective with concomitant interventions to stabilise drug or alcohol use, but treatment effects are not as large as for PTSD in the absence of drug or alcohol misuse.54 What is the prognosis in PTSD? Few longitudinal follow-up studies have been done of PTSD, but for many patients PTSD is severe and enduring.5 There is, however, good evidence that patients may benefit from treatment even when the symptoms have been present for many years.34 Are there emerging options to prevent and treat PTSD? Several experimental studies provide hope that better or alternative ways to prevent and treat PTSD are on the way. Simple visuospatial tasks such as playing a computer game shortly after a traumatic experience reduce re-experiencing.55 For established PTSD, interest in using drugs to augment psychological therapy is increasing. The results of a recent RCT of the psychedelic 3,4-methylenedioxymethylamphetamine with psychotherapy for treatment resistant PTSD have been promising.56 57 These approaches remain in their infancy, and further well designed clinical studies are required to determine if they will live up to their early promise. Contributors: JB, CL, and NR planned, conducted reviews, and drafted the article. SC drafted the patient’s perspective box and commented on and amended the initial draft. All authors reviewed and agreed the final draft. JB is the guarantor. Competing interests: We have read and understood the BMJ policy on declaration of interests and declare the following: JB, CL, and NR have For personal use only: See rights and reprints http://www.bmj.com/permissions undertaken systematic reviews, meta-analyses, randomised controlled trials, and other research in the specialty of traumatic stress, some of which is referred to in the manuscript. JB, CL, and NR are members of a research team that developed a web based guided self help programme to treat PTSD. The programme is likely to be marketed in the future. Royalties will be payable to Cardiff University, with a proportion of these being shared with the research team in line with Cardiff University’s rules. Provenance and peer review: Commissioned; externally peer reviewed. 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 Bonanno GA. Loss, trauma, and human resilience: have we underestimated the human capacity to thrive after extremely aversive events? Am Psychol 2004;59:20-8. Karstoft K, Galatzer-Levy IR, Statnikov A, Li Z, Shalev AY. Bridging a translational gap: using machine learning to improve the prediction of PTSD. BMC Psychiatry 2015;15:30. Schnurr PP, Green BL, Kaltman, S. Trauma exposure and physical health. In: Friedman MJ, Keane TM, Resick PA, eds. Handbook of PTSD: science and practice. Guilford Press, 2007. Gupta MA. Review of somatic symptoms in post-traumatic stress disorder. Int Rev Psychiatry 2013;25:86-99. Kessler RC, Sonnega A, Bromet E, Hughes M, Nelson CB. Posttraumatic stress disorder in the national comorbidity survey. Arch Gen Psychiatry 1995;52:1048-60. Sareen J, Cox BJ, Stein MB, Afifi TO, Fleet C, Asmundson GJG. Physical and mental comorbidity, disability, and suicidal behavior associated with posttraumatic stress disorder in a large community sample. Psychosom Med 2007;69:242-8. Ferry F, Bolton D, Bunting B, O’Neill S, Murphy S, Devine B. Economic impact of post traumatic stress in Northern Ireland. Northern Ireland Centre for Trauma and Transformation and University of Ulster Psychology Research Institute, 2010. Tanielian TL, Jaycox LH, eds. Invisible wounds of war: psychological and cognitive injuries, their consequences. RAND, 2009. Bisson J. Post-traumatic stress disorder. BMJ 2007;334:789-93. Muldoon OT, Lowe RD. Social identity, groups, and post‐traumatic stress disorder. Polit Psychol 2012;33:259-73. McManus S, Meltzer H, Brugha T, Bebbington P, Jenkins R, eds. Adult psychiatric morbidity in England, 2007: results of a household survey. NHS Information Centre for Health and Social Care, 2008. Alonso J, Angermeyer MC, Lépine JP. The European Study of the Epidemiology of Mental Disorders (ESEMeD) project: an epidemiological basis for informing mental health policies in Europe. Acta Psychiatr Scand 2014;109(s420):5-7. Steel Z, Chey T, Silove D, Marnane C, Bryant RA, van Ommeren M. Association of torture and other potentially traumatic events with mental health outcomes among populations exposed to mass conflict and displacement: a systematic review and meta-analysis. JAMA 2009;302:537-49. American Psychiatric Association. Diagnostic and statistical manual of mental disorders, 5th edn. American Psychiatric Publishing, 2013. World Health Organization. The ICD-10 classification of mental and behavioural disorders: clinical descriptions and diagnostic guidelines. WHO, 1992. Brewin CR, Fuchkan N, Huntley Z, et al. Outreach and screening following the 2005 London bombings: usage and outcomes. Psychol Med 2010:40;2049-57. Maercker A, Brewin CR, Bryant RA, et al. Proposals for mental disorders specifically associated with stress in the International Classification of Diseases-11. Lancet 2013;381:1683-5. White J, Pearce J, Morrison S, Dunstan F, Bisson JI, Fone DL. Risk of post traumatic stress disorder following traumatic events in a community sample. Epidemiol Psychiatr Sci 2015;24:249-57. Bisson JI. What happened to harmonisation of the PTSD diagnosis? The divergence of ICD11 and DSM5. Epidemiol Psychiatr Sci 2013;22:205-7. Kleim S, Kroger C. Prevention of chronic PTSD with early cognitive behavioral therapy. A meta-analysis using mixed-effects modeling. Behav Res Ther 2013;51:753-61. Roberts NP, Kitchiner NJ, Kenardy J, Bisson JI. Early psychological interventions to treat acute traumatic stress symptoms. Cochrane Database Syst Rev 2010;3:CD007944. Bastos MH, Furuta M, Small R, McKenzie-McHarg K, Bick D. Debriefing interventions for the prevention of psychological trauma in women following childbirth. Cochrane Database Syst Rev 2015;4:CD007194. Gartlehner G, Forneris CA, Brownley KA, et al. Interventions for the prevention of Posttraumatic Stress Disorder (PTSD) in adults After exposure to psychological trauma. Comparative Effectiveness Review No 109. AHRQ Publication No 13-EHC062-EF. Agency for Healthcare Research and Quality, Apr 2013. www.effectivehealthcare.ahrq.gov/reports/ final.cfm. Subscribe: http://www.bmj.com/subscribe BMJ 2015;351:h6161 doi: 10.1136/bmj.h6161 (Published 26 November 2015) Page 4 of 7 CLINICAL REVIEW How were patients involved in this clinical review? Sarah Cosgrove is a former patient with PTSD and a representative of the public in Cardiff University’s Traumatic Stress Research Group. Sarah is a coauthor of the paper and provides an account of her experiences in the patient’s perspective box. A patient’s perspective I was diagnosed with PTSD in November 2013 in the aftermath of a violent assault. From the time of the attack to the case coming to court, I had support from police and victim services enabling me to face my assailant in court with courage and conviction. But in the weeks after the judicial process had concluded, I started to unravel. Naturally a glass half full sort of person, I slid into a state of great anxiety, frightened to be alone, scared to be in a group, reluctant to go out, and terrified of staying at home. I knew something was very wrong. I had gone from being confident and outgoing, to not being able to sleep, being tearful, and experiencing episodes of unparalleled low mood. My GP immediately diagnosed PTSD. Being able to put a label on what I was going through was so helpful—it meant that there was something wrong. Fortunately, I was offered the chance to participate in a trial of a guided self help programme for sufferers of PTSD. This enabled me to both confront my experience and desensitise it, and within a few months I felt stronger than I had ever been. The programme has given me a coping strategy to employ whenever I get negative thoughts or flashbacks. It may have saved my life; at the very least it got me back to the person I used to be. Tips for non-specialists A traumatic event can precipitate conditions other than PTSD, such as depression, phobic anxiety, and substance use disorders PTSD is associated with comorbidity Sensitive questioning is required to elicit symptoms of PTSD as patients may avoid volunteering their traumatic experience(s) Patients with PTSD may present in primary care with physical symptoms that are difficult to explain Trauma focused psychological therapy is the treatment of choice for PTSD, although drugs and other forms of psychological treatment can help Patient choice and availability of psychological therapy will influence the treatment given When to suspect PTSD • When patients present with mental or physical symptoms that cannot be fully explained after a traumatic event • When patients present with characteristic symptoms of PTSD—re-experiencing, avoidance, and hyperarousal • When patients disclose a history of involvement in a traumatic event • When patients present with mental or physical symptoms that are difficult to explain in the absence of a disclosed traumatic event Additional educational resources Information for healthcare professionals Websites providing information on the assessment and treatment of PTSD: International Society for Traumatic Stress Studies (www.istss.org) US Department of Veterans Affairs, National Centre for PTSD (www.ptsd.va.gov) Information for patients Websites providing information on symptoms of PTSD and treatment options: NHS Choices PTSD (www.nhs.uk/Conditions/Post-traumatic-stress-disorder/Pages/Introduction.aspx) Royal College of Psychiatrists (www.rcpsych.ac.uk/expertadvice/problemsdisorders/posttraumaticstressdisorder.aspx) International Society for Traumatic Stress Studies (www.istss.org) National Centre for Mental Health (http://ncmh.info/conditions/post-traumatic-stress-disorder-ptsd/) US Department of Veterans Affairs, National Centre for PTSD (www.ptsd.va.gov/public/pages/fslist-self-help-cope.asp)—provides information on the symptoms of PTSD, self help, and treatment options 24 25 26 27 28 29 30 31 Roberts NP, Kitchiner NJ, Kenardy J, Bisson JI. Multiple session early psychological interventions for the prevention of post-traumatic stress disorder. Cochrane Database Syst Rev 2009;3:CD006869. Rose S, Bisson J, Churchill R, Wessely S. Psychological debriefing for preventing post traumatic stress disorder (PTSD). Cochrane Database Syst Rev 2002;2:CD000560. Sijbrandij M, Kleiboer A, Bisson JI, Barbui C, Cuijpers P. Pharmacological prevention of Posttraumatic Stress Disorder and Acute Stress Disorder: a systematic review and meta-analysis. Lancet Psychiatry 2015;2:413-21. Brewin CR, Andrews B, Valentine JD. Meta-analysis of risk factors for posttraumatic stress disorder in trauma-exposed adults. J Consult Clin Psychol 2000;68:748–66. Inter-Agency Standing Committee. IASC guidelines on mental health and psychosocial support in emergency settings. IASC, 2007. Bisson JI, Tavakoly B, Witteveen AB, et al. TENTS guidelines: development of post-disaster psychosocial care guidelines through a Delphi process. Br J Psychiatry 2010:196:69-74. Williams R, Bisson J, Kemp V. Principles for responding to people’s psychosocial and mental health needs after disasters. OP94. Royal College of Psychiatrists, 2014. American Psychiatric Association. Practice guidelines for the treatment of patients with acute stress disorder and posttraumatic stress disorder. APA, 2004. For personal use only: See rights and reprints http://www.bmj.com/permissions 32 33 34 35 36 37 Australian Centre for Posttraumatic Mental Health. Australian guidelines for the treatment of adults with acute stress disorder and posttraumatic stress disorder. ACPMH, 2007. National Collaborating Centre for Mental Health. Post-traumatic stress disorder (PTSD): the management of PTSD in adults and children in primary and secondary care—national cost impact report. National Institute for Health and Clinical Excellence, 2005. Bisson J, Roberts N, Andrew M, Cooper R, Lewis C. Psychological therapies for chronic post-traumatic stress disorder (PTSD) in adults (Review). Cochrane Database Syst Rev 2013;12:CD003388. Barrera TLM. A meta-analytic review of exposure in group cognitive behavioral therapy for posttraumatic stress disorder. Clin Psychol Rev 2013;33:24-32. Health Technology Assessment database. Comparative effectiveness of psychological treatments and pharmacological treatments for adults with posttraumatic stress disorder. 2011. www.effectivehealthcare.ahrq.gov/index.cfm/search-for-guides-reviews-and-reports/ ?pageaction=displaytopic&. Jonas D, Cusack K, Forneris C, et al. Psychological and pharmacological treatments for adults with posttraumatic stress disorder (PTSD). AHRQ Comparative Effectiveness Review 2013, Report No: 13-EHC011-EF. Subscribe: http://www.bmj.com/subscribe BMJ 2015;351:h6161 doi: 10.1136/bmj.h6161 (Published 26 November 2015) Page 5 of 7 CLINICAL REVIEW 38 39 40 41 42 43 44 45 46 47 48 49 Courtois CA, Ford JD. Treating complex traumatic stress disorders: an evidenced-based guide. Guilford Press, 2009. Cloitre M, Courtois CA, Charuvastra A, Carapezza R, Stolbach BC, Green BL. Treatment of complex PTSD: Results of the ISTSS expert clinician survey on best practices. J Trauma Stress 2011;24:615-27. Lewis G, Araya R, Elgie R, Harrison G, Proudfoot J. Self help interventions for mental health problems. In: Briefing DoHE, ed, 2003. Kar N. Cognitive behavioral therapy for the treatment of post-traumatic stress disorder: A review. Neuropsychiatr Dis Treat 2011;7:167-81. Van Emmerik AAP. Writing therapy for posttraumatic stress: a meta-analysis. Psychother Psychosom 2013;82:82-8. Ivarsson D, Blom M, Hesser H, et al. Guided internet-delivered cognitive behavior therapy for post-traumatic stress disorder: A randomized controlled trial. Internet Interv 2014;1:33-40. Litz BT, Engel CC, Bryant RA, et al. A randomized, controlled proof-of-concept trial of an Internet-based, therapist-assisted self-management treatment for posttraumatic stress disorder. Am J Psychiatry 2007;164:1676-83. Spence J, Titov N, Dear BF, et al. Randomized controlled trial of Internet‐delivered cognitive behavioral therapy for posttraumatic stress disorder. Depress Anxiety 2011;28:541-50. World Health Organization. WHO guidelines on conditions specifically related to stress. Geneva: WHO, 2013. Hoskins M, Pearce J, Bethell A, et al. Pharmacotherapy for post-traumatic stress disorder: systematic review and meta-analysis. Br J Psychiatry 2015;206:93-100. Leucht S, Hierl S, Kissling W, Dold M, Davis JM. Putting the efficacy of psychiatric and general medicine medication into perspective: review of meta-analyses. Br J Psychiatry 2012;200:97-106. Raskind MA, Peskind ER, Hoff DJ, et al. A parallel group placebo controlled study of prazosin for trauma nightmares and sleep disturbance in combat veterans with post-traumatic stress disorder. Biol Psychiatry 2007;61:928-34. For personal use only: See rights and reprints http://www.bmj.com/permissions 50 51 52 53 54 55 56 57 Raskind MA, Peterson K, Williams T, et al. A trial of prazosin for combat trauma PTSD with nightmares in active-duty soldiers returned from Iraq and Afghanistan. Am J Psychiatry 2013;170:1003-10. Stein MB, Kline NA, Matloff JC. Adjunctive olanzapine for SSRI-resistant combat-related PTSD: a double-blind, placebo-controlled study. Am J Psychiatry 2002;159:1777–9. Krystal JH, Rosenheck RA, Cramer JA, et al. Adjunctive risperidone treatment for antidepressant-resistant symptoms of chronic military service-related PTSD: a randomized trial. JAMA 2011;306:493-502. Hetrick SE, Purcell R, Garner B, Parslow R. Combined pharmacotherapy and psychological therapies for post traumatic stress disorder (PTSD). Cochrane Database Syst Rev 2010;7:CD007316. Roberts NP, Roberts PA, Jones N, Bisson JI. Psychological interventions for post-traumatic stress disorder and comorbid substance use disorder: a systematic review and meta-analysis. Clin Psychol Rev 2015;38:25-38. James EL, Bonsall MB, Hoppitt L, et al. Computer game play reduces intrusive memories of experimental trauma via reconsolidation-update mechanisms. Psychol Sci 2015;26:1201-15. Mithoefer MC, Wagner TM, Mithoefer AT, Jerome L, Doblin R. The safety and efficacy of ±3,4-methylenedioxymethamphetamine-assisted psychotherapy in subjects with chronic, treatment-resistant posttraumatic stress disorder: the first randomized controlled pilot study. J Psychopharmacol 2011;25:439-52. Mithoefer MC, Wagner MT, Mithoefer AT, et al. Durability of improvement in post-traumatic stress disorder symptoms and absence of harmful effects or drug dependency after 3,4-methylenedioxymethamphetamine-assisted psychotherapy: a prospective long-term follow- up study. J Psychopharmacol 2013;27:28-39. Cite this as: BMJ 2015;351:h6161 © BMJ Publishing Group Ltd 2015 Subscribe: http://www.bmj.com/subscribe BMJ 2015;351:h6161 doi: 10.1136/bmj.h6161 (Published 26 November 2015) Page 6 of 7 CLINICAL REVIEW Table Table 1| Symptoms required for diagnosis of PTSD DSM-5 criteria14 Proposed ICD-11 criteria17 Intrusion symptoms Recurrent, involuntary and intrusive distressing memories Recurrent distressing dreams (content and/or affect related) Dissociative reaction (acting or feeling as if event is recurring) Vivid intrusive memories, flashbacks, or nightmares, typically accompanied by strong and overwhelming emotions such as fear or horror, and strong physical sensations Intense or prolonged psychological distress to cues Noticeable physiological reactions to cues Avoidance Avoidance or efforts to avoid distressing thoughts or feelings about or closely associated Avoidance of thoughts and memories of the event or events with the trauma Avoidance of activities, situations, or people reminiscent of the event Avoidance or efforts to avoid external reminders (people, places, conversations, activities, or events objects, situations) Negative alterations in cognitions and mood Inability to remember an important aspect (typically due to dissociative amnesia) Not applicable Persistent and exaggerated negative beliefs or expectations about oneself, others, or the world (for example, “I am bad,” “No one can be trusted,” “The world is completely dangerous”) Persistent, distorted cognitions about the cause or consequences that lead to self blame or the blame of others Persistent negative emotional state (for example, fear, horror, anger, guilt, shame) Noticeably diminished interest or participation in important activities Feelings of detachment or estrangement from others Persistent inability to experience positive emotions (for example, happiness, satisfaction, love) Alterations in arousal and reactivity Irritable behaviour and angry outbursts (with little or no provocation) Reckless or self destructive behaviour Hypervigilance Persistent perceptions of heightened current threat—for example, as indicated by hypervigilance or an enhanced startle reaction to stimuli such as unexpected noises Exaggerated startle response Problems with concentration Sleep disturbance Additional criteria for complex PTSD Not applicable Severe and pervasive problems in affect regulation Persistent beliefs about oneself as diminished, defeated, or worthless, accompanied by deep and pervasive feelings of shame, guilt, or failure related to the stressor Persistent difficulties in sustaining relationships and in feeling close to others For personal use only: See rights and reprints http://www.bmj.com/permissions Subscribe: http://www.bmj.com/subscribe BMJ 2015;351:h6161 doi: 10.1136/bmj.h6161 (Published 26 November 2015) Page 7 of 7 CLINICAL REVIEW Figure Examples of the many different trajectories of PTSD symptoms after exposure to trauma For personal use only: See rights and reprints http://www.bmj.com/permissions View publication stats Subscribe: http://www.bmj.com/subscribe